CONDITIONS F - O
These pages offer explanations of pediatric medical surgical conditions including:
- what the condition is
- signs and symptoms
- how it is diagnosed
- treatment
- home care
- long-term outcomes
Use it as a reference when discussing your child’s individual condition and treatment with your doctor and medical professionals.
Fistula-in-Ano
Condition: Fistula-in-Ano (peri-anal abscess or sinus tract)
Overview (“What is it?”)
- Definition: A fistula-in-ano (also known as perianal fistula) is an abnormal connection between the anal canal and the skin around the anus. A perianal abscess is a collection of pus or infection near the anus. These two conditions often occur with each other.
- Epidemiology: Fistula-in-ano occurs most commonly in infants younger than one year of age. A fistula-in ano is usually caused by an infection or abscess.
Signs and Symptoms (“What symptoms will my child have?”)
- Early signs: The first sign of a perianal fistula is a perianal abscess which is a tender, red mass around the anus in an infant.
- Later signs/symptoms: If left untreated, the abscess can get bigger and the baby can have fevers. Sometimes, the abscess can pop open and drain. If the abscess has an associated fistula, recurrent abscesses or a small draining opening at the same site can happen.
Diagnosis (“What tests are done to find out what my child has?”)
- A perianal abscess can be diagnosed by physical exam. To identify whether there is an associated fistula, sedation or anesthesia is needed.
- Labs and tests: No labs are typically necessary in infants with a fistula. In older children (above toddler age), a perianal abscess or fistula may signify an intestinal inflammatory process (inflammatory bowel disease). Further workup is needed in an older child.
- Conditions that mimic this condition: Perianal abscess without fistula; inflammatory bowel disease.
Treatment (“What will be done to make my child better?”)
- Medicine: Your child may be given medicine for pain and for any fevers (Acetaminophen [Tylenol®] or Ibuprofen [Motrin®]). You may also be given an antibiotic, which is a medicine to treat the infection.
- Surgery: Drainage of the abscess may be all that is necessary for some children who present with a perianal abscess and no obvious fistula If the abscess returns, alternatives include repeat drainage of abscess or a fistulotomy (unroofing of the sinus tract) may be performed. This is typically an outpatient procedure, and your child should be able to come home the same day.
-
- Preoperative preparation: Your child will have to have an empty stomach for several hours prior to anesthesia. Intravenous (IV) antibiotics may be given just before surgery.
- Postoperative care: You will likely be instructed to begin bathing your child in warm, soapy water after each bowel movement to keep the wound clean. You may be asked to continue antibiotics and pain medications. For either drainage of abscess or unroofing of fistula, the wound needs to heal from the bottom up. It takes a few days (1-2 weeks) for the wound to completely heal over.
- Risks/Benefits:
- Risks of surgery include bleeding, infection and recurrence of the wound.
- Risks of not treating the abscess or fistula is progression of infection which may spread to the surrounding skin or into the bloodstream.
- Most often, drainage of abscess solves the problem. If the abscess recurs multiple times, then a fistulotomy would solve the issue.
Home Care (“What do I need to do once my child goes home?”)
- Diet: There are no dietary restrictions.
- Activity: There are no activity restrictions.
- Wound care: Bathe in warm, soapy water after each bowel movement until the wound is healed (typically 1-2 weeks).
- Medicines: Prescriptions for antibiotics and pain medications may be prescribed.
- What to call the doctor for: Call for persistent fevers, increasing pain or increasing redness around the wound.
- Follow-up care: You may follow up with your pediatrician or surgeon 1-2 weeks after fistulectomy to make sure the wound is healing appropriately.
Long-Term Outcomes (“Are there future conditions to worry about?”)
Once the fistula is removed, the chance of recurrent problems is very low. Recurrent abscesses or fistulas after adequate treatment will need further studies to determine the underlying cause.
Updated: 11/2016
Author: Patricia Lange, MD
Editor: Marjorie J. Arca, MD
Gallbladder Diseases
Gallbladder Diseases:
Condition:
Cholelithiasis (gallstones)
Choledocholithiasis (stones in the bile duct)
Cholecystitis (infection of the gallbladder)
The gallbladder is an organ located underneath the liver in the upper right part of the belly just below the ribcage. The liver makes bile and gallbladder normally stores bile. In response to a meal, the gallbladder releases bile released into the small intestine to aid in breaking down (digestion) of foods. The bile that travels through the intestines makes the stool yellow, green or brown. Here, we discuss conditions that can affect the gallbladder.
Overview (“What is it?”)
- Definition: Cholelithiasis refers to stones in the gallbladder (“gallstones”).
- Epidemiology: Up to 30% of the adult population have gallstones. Overall, gallstones are less common in children . Stones tend to form in the gallbladder when the bile has a higher concentration of cholesterol and bilirubin. Cholesterol is something that can be found in fatty foods and a diet has a high fat content can contribute to gallstone formation. Bilirubin is a substance that the body forms when the red cells in the blood are processed by the body. So, in conditions when there is a high rate of blood turnover, more bilirubin is made and needs to be handled by the liver. The bilirubin level is higher in the bile and can lead to gallstones. Conditions that have a high red blood cell turnover include occur for a variety of reasons. These conditions include sickle cell anemia, hereditary spherocytosis and beta-thalessemia. Up to 50% of children with sickle cell anemia will develop gallstones by 20 years of age.
- There are other risk factors that seem to be associated with gallstone formation. In children and adolescents, obesity, pregnancy, use of birth control pills, and cystic fibrosis are risk factors for this problem. Over 40% of babies who needed to nutrition to be given through the vein (total parenteral nutrition or TPN) will develop gallstones. Before puberty, gallstones are equally likely in boys and girls, but after puberty girls are more likely to have gallstones.
- Choledocholithiasis (choledocho – bile ducts, lithiasis – stones) is the condition when stones from the gallbladder get stuck in the bile duct between the gallbladder and the small intestine. This can cause yellowing of the skin (jaundice) and sometimes, an infection of the bile ducts and liver.
- Cholecystitis—is an infection of the gallbladder that can be associated with gallstones.
Signs and Symptoms (“What symptoms will my child have?”)
- Early signs: Include belly pain and/or nausea after eating, especially if the food is high in fat. The gallbladder squeezes bile after a meal, and having stones in the gallbladder can cause pain. The pain can be sharp or dull like an ache. It is usually the right upper side of the belly, just below the rib cage, or spread to the right shoulder or right middle back. Older children are better able to narrow down their symptoms. Younger children may have a hard time describing their pain, so making the diagnosis in young children can be tough.
- Sometimes, small gallstones can come out of the gallbladder as the gallbladder squeezes. These stones can get stuck within the bile duct system between gallbladder and the small intestine. If this happens, a number of serious problems can happen. These include blockage of bile flow into the small intestine, causing jaundice, pale colored stools and dark brown urine. If the stones go even lower down in the bile duct, they can block the duct of the pancreas and cause inflammation of the pancreas (pancreatitis). Another possible complication is infection of the bile ducts (cholangitis). This infection can lead to high fevers.
- Gallstones can lead to infections of the gallbladder. In this case, fever may accompany nausea, vomiting, and belly pain.
Diagnosis (“What tests are done to find out what my child has?”)
- Physical examination by a doctor
- Blood tests: including white blood cell count to look for infection, blood test to check function of the liver and pancreatic enzymes to rule out pancreatic inflammation
- Abdominal X-ray: only detects 30% of stones. Sometimes X-rays are done to make sure that there are no other possible causes of pain.
- Ultrasound: best test to look gallstones. Ultrasound can also detect whether an infection of the gallbladder is present. If dilation of the bile ducts are seen, this may give a clue that stones are stuck in the bile duct. Most of the time, an ultrasound is the only test needed.
- HIDA scan: (also known as cholescintigraphy or hepatobiliary scintigraphy) is a test that outlines the path that bile follows. In this test, a tracer is injected into the blood of the child. Like bile, this tracer is taken up by the liver and is concentrated in the gallbladder, goes through the bile duct, and is emptied to the small intestine. If the patient has infection of the gallbladder, the tracer may not go to the gallbladder. If there is a blockage of the bile duct, then the tracer won’t go into the small bowel. This test is not used commonly since ultrasound is effective.
- CT scan: is not helpful for diagnosis gallstones in children. If other problems are being checked out or if there is worry of pancreatic inflammation, a CT may be useful.
Treatment: (“What will ne done to make my child better?”)
- Medical Options: There are very few medical options to treat gallstones.
- Ursodeoxycholic acid – is a medicine that may be given to dissolve gallstones, but there is a high risk that the gallstones will come back.
- Decreasing risk factors to prevent gallstone formation is helpful. In infants, limiting the use of TPN may help with gallstone formation. In older children, preventing obesity with a healthy diet low in fat and regular exercise is helpful.
- Observation without intervention is indicated if there are no symptoms from gallstones. Sometimes, gallstones stones caused by TPN can resolve within 6-12 months.
- Endoscopy: If doctors think that there are stones stuck in the bile duct (choledocholithiasis), they may recommend a procedure to remove the stones first. The procedure is called Endoscopic Retrograde Cholangiopancreatography or ERCP, for short. An ERCP involves using a telescopic camera inserted through the mouth, passed through the stomach and the small intestine. Since the bile duct empties into the small intestine, the duct can be seen and approached in this region. To remove the stone, a small cut is made at the entry site of the duct (sphincterotomy) and small balloons are used to clear stones from the duct. The stones go into the small intestine and is naturally passed through the stool.
- Surgery is the best and only treatment for gallstones that cause symptoms. The gallbladder and the stones within it are removed. Commonly, the surgery is done laparoscopically. In “laparoscopic surgery”, several small cuts (incisions) are made. Through one of the cuts, a video camera is placed. The surgery itself if done using small instruments placed through the other incisions. Sometimes, the surgeon might think that it is a good idea to define the bile duct anatomy. This is done by injecting dye into the bile ducts. This may show if there are stones in the duct or if there is injury to the bile duct. If stones are found in the duct, the surgeon may do maneuvers to clear the duct. If the duct cannot be cleared at the time of the operation, an ERCP may be necessary after surgery.
- Although most gallbladder removal surgeries are done laparoscopically, there may be times when a big incision is necessary. Some of the reasons for this include too much inflammation, inability to clear the duct using laparoscopy, or the anatomy of the gallbladder and the bile duct is not clear.
- Preoperative preparation consists of care to make your child as healthy as possible before surgery. If gallbladder infection is present, your child may be given antibiotics before surgery is completed. In the case of the child with sickle cell anemia, blood transfusions may be required before surgery to prevent a sickle cell crisis. Patients are usually asked to shower or bathe on the night before surgery. Patients are asked to stop eating or drinking for a few hours before surgery.
- Postoperative care consists of pain management and wound care. If the procedure is done laparoscopically, most children can go home on the day of the surgery or the following day. If a bigger incision is needed, there is more pain and so the patient needs to stay the hospital longer, with an average of 5-7 days after surgery.
- Risks of ERCP include pancreatic inflammation, bleeding from sphincterotomy site (cut from the bile duct opening), hole in the intestine. Pancreatic inflammation usually gets better in 24-48 hours. Bleeding from sphincterotomy site may require another ERCP or surgery. A hole in the intestine can be managed with antibiotics alone or may need surgery depending on how big the hole is and how sick the patient is.
- Risks of laparoscopic cholecystectomy include damage to the common bile duct, leakage of bile, bleeding, wound infection, retained stone in the bile duct. Whenever laparoscopic surgery is performed, there is always a chance that the surgery may be converted to open surgery (larger incision in the abdomen). Some of these complications can require further surgery.
- Benefit of surgery is relief of pain from gallstones. If infection and/or bile duct blockage is presents, these problems are also solved.
Home Care (“What do I need to do once my child goes home?”)
- Diet: Your child may eat a normal diet after surgery. Sometimes, eating lots fatty foods may result loose stools and cramping. These problems will likely go away after several months as the body adjusts to not having a gallbladder.
- Activity: Your child should avoid strenuous activity and heavy lifting for the first 1-2 weeks after laparoscopic surgery, 4-6 weeks after open surgery.
- Wound Care: Surgical incisions should be kept clean and dry for a few days after surgery. Most of the time, the stitches used in children are absorbable and do not require removal. Your surgeon will give you specific guidance regarding wound care, including when your child can shower or bathe.
- Medicines: Medicines for pain such as acetaminophen (Tylenol) or ibuprofen (Motrin or Advil) or something stronger like a narcotic may be need to help with pain for a few days after surgery. Stool softeners and laxatives are needed to help regular stooling after surgery, especially if narcotics are still needed for pain.
- What to call the doctor for: Call your doctor for worsening belly pain, fever, vomiting, jaundice or If the wounds are red or draining fluid.
- Follow up care: Your child should follow-up with his or her surgeon 2-3 weeks after surgery to ensure proper post-operative healing. You should continue to see your pediatrician regularly to address and manage the primary cause of your child’s gallstones (examples: obesity, hemolytic anemia, cystic fibrosis)
Long Term Outcomes (“Are there future conditions to worry about?”)
- After surgical treatment, the long-term prognosis is excellent.
- Few patients may feel like vomiting and bloated after eating fatty foods. This is usually temporary. Follow-up with your pediatric surgeon if your child experiences these symptoms.
References:
Articles and graphics adapted from:
O’Neill: Principles of Pediatric Surgery. © 2003, Elsevier.
Holcomb: Ashcraft’s Pediatric Surgery, Sixth Edition. © 2014, Elsevier Inc.
Coran: Pediatric Surgery, Seventh Edition © 2012, 2006 by Saunders, an imprint of Elsevier Inc.
Svensson J, Makin E. Gallstone disease in children. Semin Pediatr Surg. 2012 Aug. 21(3):255-65.
NIH Medline, https://www.nlm.nih.gov/medlineplus/ency/article/000273.htm
Article and tables adapted from Coran: Pediatric Surgery. Ó2012, Elsevier.
Updated: 11/2016
Author: Marjorie J. Arca, MD
Editors: Marjorie J. Arca, MD, R. Ignacio, MD, L. Kiss, MD, M. Vu, MD
Gastrointestinal Foreign Bodies and Bezoars
Condition: Gastrointestinal Foreign Bodies and Bezoars (intestinal foreign bodies)
For objects in the esophagus, please see esophageal foreign bodies, injury and trauma.
Overview (“What is it?”)
- Children place objects in their mouths and accidentally or intentionally swallow them. Objects may be stuck in any part of the digestive tract from the throat to the intestines, causing blockage. Some items may also cause direct injury to the intestine; for instance, disc batteries may damage the esophagus, magnets may create holes in the intestine and sharp objects can tear surrounding tissue. A bezoar is a solid mass of indigestible material that is usually stuck in the stomach. These materials include vegetable matter, fruits, vegetables, seeds or hair. A bezoar can occupy most of the inside of the stomach and may even extend to the small intestine.
- Ingestion of objects most commonly happens in toddlers, as they are exploring their surroundings and often place objects into their mouths.
- In adolescents who have meat stuck in their esophagus, the diagnosis of eosinophilic esophagitis should be ruled out.
Signs and Symptoms (“What symptoms will my child have?”)
- Early signs: When an object is stuck in the esophagus, chest pain may be felt. If the flow of saliva is obstructed, the child may drool. If there are indigestible material in the stomach, vomiting can be a symptom.
- Later signs/symptoms: If the bezoar in the stomach is large, the mass may be felt on abdominal exam, especially if the child is thin. The child may have belly pain and get full easily. Obstruction or blockage of the intestine can result in vomiting of bile (green or yellow in color).
Diagnosis (“What tests are done to find out what my child has?”)
- Labs and tests: Metallic objects are visible on plain X-rays and their location may be seen. Depending on the symptoms of the patient, a computed tomography (CT scan) may be needed. This specialized X-ray may give a better answer regarding the type of object and the level of obstruction or any other problems that the object has caused.
- Conditions that mimic this condition: Some infections of the throat (pharyngitis), neck and intestines (gastroenteritis) may simulate a foreign body ingestion. Reflux can also cause similar problems. Intestinal blockage caused other reasons (inflammation, scarring) can have the same symptoms.
Treatment (“What will be done to make my child better?”)
- Medicine: Pain medication may be given if your child is uncomfortable. If the child requires surgery, medications to treat infection (antibiotics) may be given.
- Surgery: The type of procedure varies depending on the type of object, location of the object, and what problems the object has caused.
- Small objects in the stomach may be retrieved by endoscopy. Endoscopy is when a flexible telescope is placed in the mouth and is gently pushed through the esophagus, stomach and part of the small intestine. The doctor can look at evidence of damage or injury directly. If there is an object stuck in the stomach, it is removed during this procedure. Most coins will pass through the intestinal tract once they are in the stomach and usually do not require endoscopic retrieval. However, open safety pins, objects with sharp edges and items that fail to go through the stomach will need to be removed.
- Your child may require an operation if: (1) endoscopy fails to retrieve the object from the stomach; (2) object migrated to the intestine and is stuck; or (3) other complications have resulted from the object. The operation can be done the traditional way (“open” or larger incision) or laparoscopic.
- Open: The operation is done through a large incision belly, usually up and down (vertical).
- Laparoscopy: In laparoscopy surgery, several small cuts (incisions) are made. Through one of the cuts, a video camera is placed. The surgery itself is done using small instruments placed through the other incisions.
- The approach and exactly what will be done at the operation will be discussed with you by the surgeon and the surgical team.
- Preoperative preparation: Your child will not be allowed to eat prior to the time of surgery. If the child requires surgery, medications to treat infection (antibiotics) may be given.
- Postoperative care: Depending on what is done, your child may be sent home shortly after the foreign body is removed (if no cut was needed) or s/he may need to stay in for several days to allow the cuts to heal and the intestines to start working.
- Risks/Benefits
- Risks: Endoscopy may cause injury of the esophagus. The child may aspirate saliva or contents of the stomach into the lungs. Risks of surgery include bleeding, infection and injury to organs.
- Benefits: Removal of a foreign body often gives immediate relief of symptoms. Endoscopy can show how bad the injury can be. If surgery is required, removal of the object and dealing with complications will be accomplished.
Home Care (“What do I need to do once my child goes home?”)
- Diet: Your child should be able to resume a general diet.
- Activity: If endoscopy was performed, the child should be able to resume normal activity right away. If the patient had the procedure with small incisions (laparoscopic), he or she can be back to normal activity in 1-2 weeks. If the surgery is done through a big incision, then he or she can be back to normal activities in six weeks, with a weight restriction of 10 pounds up until that time.
- Wound care: The patient can shower in three days but may want to wait 5-7 days after surgery before soaking the wound.
- Medicines: Medication for pain such as acetaminophen (Tylenol®) or ibuprofen (Motrin® or Advil®) or something stronger like a narcotic may be needed to help with pain for a few days after surgery. Stool softeners and laxatives are needed to help regular stooling after surgery, especially if narcotics are still needed for pain.
- What to call the doctor for: After discharge from surgery, problems that may indicate infection such as fevers, wound redness and discharge should be addressed If there is a lot vomiting, pain not getting better with pain medications, problems stooling, the surgeon should be contacted.
- Follow-up care: If your child did not need surgery to deal with the problem, it is unlikely that your child will need to be seen by the surgeon again. If a cut was made, your surgeon may want to see your child back to check the wound.
Long-Term Outcomes (“Are there future conditions to worry about?”)
Generally, the outcomes are excellent, as most are removed without incisions. If incisions are needed, the wounds usually heal very well and no long-term issues occur. The only issue to watch for is scar tissue that might form on the bowel, which may lead to the bowels being unable to pass materials forward (obstruction). Your child will most commonly present with vomiting green (bilious) material. If this happens, your child will need to be seen. If your child ingested materials such as hair, psychosocial issues will need to be addressed to prevent this from happening again. This will most likely have been arranged before your child left hospital.
Updated: 11/2016
Author: Kenneth W. Gow, MD
Editors: Patricia Lange, MD; Marjorie J. Arca, MD
Gastroschisis
Condition: Gastroschisis (abdominal wall defect or hole)
Overview (“What is it?”)
- Definition: Gastroschisis occurs as your baby is developing (fetus), and a hole in the muscle and skin of the belly (abdomen) forms. Most commonly this occurs just to the right of the umbilical cord. Because the abdominal wall keeps all of the abdominal organs contained, if there is a hole, then these organs may come out. As your baby is floating in fluid (amniotic), the organs are in contact with this fluid and become irritated by it. It is not known why gastroschisis occurs.
 Figure 1: Gastroschisis. Picture courtesy of MJArcha 11/2016
Figure 1: Gastroschisis. Picture courtesy of MJArcha 11/2016
- Epidemiology: Gastroschisis occurs in 3-4 per 10,000 births. There is an association between gastroschisis and a young mother (20 years or younger).
Signs and Symptoms (“What symptoms will my child have?”)
- Early signs: If you are getting ultrasounds during pregnancy, your doctor may see this problem before birth. It is important to know that your baby does not have pain from this. However, your doctors may be watching the thickness of the intestine wall during follow-up ultrasounds to make sure that the intestine is not being damaged.
- Later signs/symptoms: Gastroschisis may be detected after your child is born. The most common organ that comes out of the hole is the intestines. Sometimes, other organs can also go through the hole.
Diagnosis (“What tests are done to find out what my child has?”)
- Labs and tests: In most instances, gastroschisis will be detected with prenatal ultrasounds, so further tests are usually not necessary after birth.
- Conditions that mimic this condition: The other abdominal wall hole which is may look like gastroschisis is called omphalocele. Unlike gastroschisis, omphaloceles occur within the belly button (umbilicus), and the internal organs are covered by a thin sac.
Treatment (“What will be done to make my child better?”)
- A baby with gastroschisis should deliver in a hospital that has ready access to surgeons and specialists that can take care of the baby right away (usually a dedicated children’s hospital). Your obstetric doctor will discuss options about delivery. The best time for delivery is not known. Most doctors believe that a baby with gastroschisis should be born close to term. Vaginal delivery is a very safe option and a Caesarian section (C-section) is not needed. However, you and your doctor should discuss what is best for your individual situation. Ideally, the parents can meet with surgeons and infant specialists before the baby is born to get an idea where and how your child will be cared for.
- Surgery
- Preoperative preparation: After delivery, your baby will have a tube passed into the stomach to make sure fluid and air are drained and so the bowels do not expand. Your baby will likely need an intravenous (IV) to get fluids as s/he may lose fluid from the exposed bowel. To keep the bowel from being injured, your baby will have the lower body placed into a plastic bag with moisture. Your child will be rapidly brought to the closest neonatal intensive care unit (NICU) for further care.
- Operative care: Surgeons will look at the hole in the abdominal wall to get an idea as to its size and whether the bowels can be put back inside. Based on the baby’s size and condition, how much intestine is out, and the condition of the intestines, the surgeon may decide whether the closure can be done at the bedside in the NICU or the operating room. The surgeon will make a decision whether putting all the organs that are outside will fit inside the belly cavity right away. If all the abdominal contents can be placed back inside without compromising the blood supply to the internal organs, then the surgeon will close the hole. If the surgeon cannot get all of the contents back into the abdomen, then the bowels will be put into a temporary bag (silo) and allow gravity to get all of the bowel back into the abdomen over a period few days, after which your surgeon will close the hole. The figure below shows a baby with gastroschisis, whose intestines are contained in a silo.
- Postoperative care: Because the intestines were exposed while developing in the uterus, they do not function normally for several days to weeks. Your baby will need to have nutrition given through his/her veins. After the bowel starts working, feeding will start and slowly advance. You can expect your baby to stay in the hospital for about a month or longer depending on how long it takes to get to full feeds. Some babies may need to be on the ventilator (breathing machine) to help with breathing for a few days after birth, especially if s/he needed to go to the operating room.
- Risks/Benefits
- Benefits: Getting all of the organs back into the abdomen and the hole closed is important because the bowel may otherwise get injured.
- Risks: If all of the intestine were placed in the abdomen and the space is too tight, blood supply to the intestines and the rest of the contents of the belly may be cut off. Other risks include wound infection and injury to the organs.
- Associated Issues: Up to one-third of babies with gastroschisis may experience an intestinal infection called necrotizing enterocolitis. Care must be exercised when advancing feeding in gastroschisis babies. About 10-15% of babies with gastroschisis can have intestinal atresia, where the intestine is not in continuity. In a small fraction of this babies, there is massive loss of intestine while inside the uterus resulting in “short gut syndrome”. In cases of atresia, repair is done weeks after birth, prolonging the hospital stay. Babies with short gut syndrome require long-term and intensive medical and surgical care. Uncommonly, babies with gastroschisis can have problems with intestinal movement and ability to digest and absorb nutrients.
Home Care (“What do I need to do once my child goes home?”)
- Diet: By the time your baby comes home, s/he should be on a full diet with no restrictions.
- Activity: There will be no activity restrictions.
- Wound care: Your surgeon will review with you details on the wound care, as it depends on the way that the hole was closed.
- Medicines: There are usually no medicines that are needed for uncomplicated gastroschisis.
- What to call the doctor for: If your baby is not keeping feeds down (throwing up), the incision or the belly button is red, please call your doctor.
- Follow-up care: You will need to be followed by your surgeon for at least one wound check after discharge and with your pediatrician for normal baby visits, especially to follow weight gain.
Long-Term Outcomes (“Are there future conditions to worry about?”)
In majority of cases, you can expect to have your baby tolerate all feeds and not have any issues. However, in cases of babies with atresia, history of NEC, problems with motility or absorption, or short gut syndrome, care at home can be very complex.
Updated: 11/2016
Author: Kenneth W. Gow, MD
Editors: Patricia Lange, MD; Marjorie J. Arca, MD
Gastroesophageal Reflux Disease
Condition: Gastroesophageal Reflux Disease
Overview (“What is it?”)
- Gastroesophageal reflux disease (also known as GERD) is a digestive condition where acid from the stomach contents flows back upward into the esophagus and, sometimes, back into the mouth leading to various symptoms.
- GERD commonly occurs due to a malfunction of barriers that normally prevent stomach contents from flowing from the stomach back up the digestive tract.
- Reflux of food (spitting up) is very common in infants. This largely resolves by 12 months of age.
- Simple reflux is different that gastroesophageal reflux disease, which is notable for associated complications or symptoms. Long-standing reflux can lead to damage of the esophagus, difficult or painful swallowing or asthma-type symptoms.
Signs and Symptoms (“What symptoms will my child have?”)
- Symptoms of GERD may vary with a child’s age. Many of the symptoms of GERD may be associated with other medical and developmental conditions. These symptoms should be discussed with a health care provider.
- Infants may fail to gain weight (also termed failure to thrive), refuse to eat, aspiration (where food or liquid come up and enter the airway instead of the esophagus), recurrent pneumonias (infections of the lungs), or esophagitis (inflammation of the esophagus).
- Preschool children may have decreased food intake, poor weight gain or respiratory problems.
- Older children and adolescents may complain of heartburn, spitting up food, hoarseness, nausea, pain in the upper abdomen, difficulty swallowing, wheezing or breathing issues.
Diagnosis (“What test are done to find out what my child has?”)
- Gastroesophageal reflux is often diagnosed based on the patient’s symptoms. A doctor or health care provider can evaluate your child for this condition.
- Additional tests may be necessary.
- Upper gastrointestinal studies: X-rays test where the child swallows contrast to evaluate the passage of food or liquid. It also shows the anatomy of the inside of the esophagus and stomach.
- Endoscopy: A diagnostic test where a physician passes a lighted flexible camera through the mouth and into the stomach while the child is sedated.
- pH Probe study: Where a catheter is inserted through the mouth, esophagus and stomach. The catheter measures the acidity of the fluid in the esophagus and stomach. This is usually done over 24 hours.
- Motility and manometry test: The movement and pressures within the esophagus is tested by catheters.
- If your child has persistent symptoms or worsening problems, seek medical evaluation by a doctor who will evaluate the symptoms.
Treatment (“What will be done to make my child better?”)
- Treatment of GERD in children and adolescents is similar to that used for adults.
- A group of medications called proton pump inhibitors (PPIs) decrease the amount of acid produced by the stomach. By lessening acidity of the the stomach, the irritation of the esophagus is reduced.
- Another group of medications, called histamine type 2 receptor agonists (also known as H2 blockers) may be also useful. These also decrease acidity of stomach fluid.
- Antacids may also be useful when symptoms are infrequent.
- All these medications are available over the counter, but use in children is best discussed with a health care provider first.
- Severe cases of GERD that do not respond to medical therapy may require surgery.
- Indications for surgery include: Pulmonary complications, inadequate response to medical management, growth failure and ongoing pain or esophagitis (damage to or narrowing of esophagus from acid).
- The most common surgery for GERD is a fundoplication, which involves wrapping a portion of the stomach around the esophagus. There are variations in how much of the esophagus is covered by the stomach and whether the stomach wraps around the front or the back. This procedure can be done laparoscopically (with several small incisions) or through a traditional larger incision. Outcomes are similar for both procedures. Depending on the child’s specific needs, a feeding tube may be placed in the stomach at the same surgery.
- The role of surgery is best determined in consultation with a pediatric surgeon.
Prevention
- There is no prevention for GERD. There are however, simple lifestyle modifications that may improve mild cases.
- For infants, there are some changes in diet that can decrease the severity of symptoms:
- Trials of smaller volume, but more frequent meals
- Elimination of cow’s milk from the diet
- Thickening of foods with infant oat or rice cereal
- Continuation of breast feeding in infants who are currently breast feeding
- For children and adolescents, the following changes can improve GERD symptoms:
- Elimination of chocolate, peppermint, carbonated or acidic beverages or any foods that seem to worsen symptoms
- Weight loss in overweight children and maintenance of appropriate weight
- Remaining upright (sitting or standing) for a period of time after meals
- Chewing gum or using lozenges
Long-Term Outcomes (“Are there future conditions to worry about?”)
- Lifestyle modifications may provide relief for patients with mild symptoms. They are useful adjuncts to medications and surgery in patients who require these therapies but are unlikely to reverse existing damage to the esophagus on their own.
- Medical management with PPIs is the usual first course of treatment. PPIs have a higher rate of medication compliance and may better aid in regression of existing damage to the esophagus as well as symptom improvement. The majority of patients respond to medical therapy along with lifestyle modifications.
- Surgery may be a reasonable alternative to long-term medication use or for those who fail to respond to medical therapy, though ongoing medical therapy may be required. A discussion with your pediatrician and surgeon should discuss the indications, risks and benefits of operative therapy.
References
- Uptodate.com: http://www.uptodate.com/contents/management-of-gastroesophageal-reflux-disease-in-children-and-adolescents?source=search_result&search=gerd+children&selectedTitle=2%7E150 http://www.uptodate.com/contents/clinical-manifestations-and-diagnosis-of-gastroesophageal-reflux-disease-in-children-andadolescents?source=search_result&search=gerd+children&selectedTitle=3%7E150.
- Holcomb, George W III, et al. Ashcraft’s Pediatric Surgery. New York. Elsevier, 2014. E-book.
- McMillan, Julia A, et al. Oski’s Pediatrics. Philadelphia. Lippincott, Williams and Wilkins, 2006. E-book.
Updated: 11/2016
Authors: J. Liebig, MD; Romeo C. Ignacio, Jr., MD
Editors: Patricia Lange, MD; Marjorie J. Arca, MD
Gynecomastia
Condition: Gynecomastia
Overview (“What is it?”)
- Gynecomastia is a benign (not cancer) enlargement of the male breast because of overgrowth of breast tissue.
- Gynecomastia may or may not cause symptoms. During some stages of childhood, it is fairly normal finding and will go away on its own. Gynecomastia is caused by many reasons including an imbalance of hormones such as estrogen, testosterone and thyroid hormone. Several medications may cause gynecomastia including some antibiotics, anti-ulcer medications, heart medicines and psychoactive medications. It has also been associated with the use of alcohol and drugs such as marijuana and amphetamines. Sometimes the cause is not clear. When gynecomastia fails to go away on its own after 1-2 years and no obvious cause is found, surgical treatment is often considered.
Signs and Symptoms (“What symptoms will my child have?”)
- Gynecomastia usually occurs in both breasts but may occur on only one side. True gynecomastia is a firm, disc-like mass beneath the nipple that may be tender. While breast cancers can occur in males, cancer is rare and unusual in the children and teenagers. Very often gynecomastia will go away on its own or after stopping any associated medications. If it persists, it tends to become more firm over time. There may be some pain, but some may not be painful. Some children have problems with body image and may find it difficult to participate in activities such as swimming where they have to remove their shirts.
Diagnosis (“What tests are done to find out what my child has?”)
- The doctor will conduct history and good physical examination including testicular exam must be done. It is important to give a list of all medications that the child is taking.
- Blood tests are conducted to see if there is a cause of the gynecomastia including tests for liver, kidney and thyroid function and hormone levels (testosterone, estradiol, prolactin, luteinizing hormone, and human chorionic gonadotropin). If all these tests are normal, then idiopathic gynecomastia is diagnosed (which means we do not know the cause).
- Conditions that mimic this problem: “Pseudogynecomastia” (false gynecomastia) which is caused by increased fat rather than breast tissue enlargement. Boys and men with pseudogynecomastia are reassured that nothing serious is happening and if treatment is requested, weight loss and possibly liposuction are recommended.
Treatment (“What will be done to make my child better?”)
- Usually pubertal gynecomastia goes away by itself within 1-2 years.
- Medical Therapy: If the child is taking medicines that potentially cause breast enlargement, they should be withdrawn or changed if possible. Over-the counter-medications such as acetaminophen (Tylenol®) and ibuprofen (Motrin®, Advil®) can be used for occasional pain.
- Surgery: Surgery may be needed if gynecomastia persists after one to two years, for pain, or if there are psychologic problems. Surgery for persistent gynecomastia involves removal of the breast tissue. This is done through a small incision either through the areola or just beneath it at the junction between the dark and lighter skin. All of the breast tissue is removed. Complete surgical removal of the breast tissue cures the condition. Because removal of the breast tissue leaves a large empty space beneath the skin, many surgeons will leave a drain in place to collect fluid after the surgery.
- Preoperative preparation: The child should shower or bathe the day before or the morning of surgery. He should not eat anything solid for eight hours prior to surgery
- Postoperative care: Depending on how extensive the operation is, the child may need to stay overnight. If a drain is placed, its care would be taught before discharge. You will need to record the volume of what is coming out of the drain. The drain will be removed in clinic when there is not much drainage left. Pain medication will be provided. Some surgeons may wrap the chest with an elastic wrap to help prevent a collection of fluid forming in this space (called a seroma) and activity in the arm on the side of the operation may be limited for a period of time after surgery.
- Benefits/Risks
- Benefits: The procedure will remove the breast tissue, which will make the chest flat.
- Risks: The main risks of the surgery are seroma formation and hematoma (blood clot) caused by any postoperative bleeding. This is not common. The surgeon has to leave a small amount of breast tissue beneath the nipple to prevent nipple inversion after surgery. Another possible risk is wound infection. Cosmetically, the chest may be asymmetric.
Home Care (“What do I need to do once my child goes home?”)
- Diet: Most children will be able to eat normally after the anesthesia has worn off. There are no dietary restrictions to follow.
- Activity: Excessive activity in the arm on the side of the operation may be limited by your surgeon for a period of weeks to help decrease the risk of seroma formation. If a drain was placed, you will need to learn how to empty it and record the amount of drainage. Usually this amount is small. Children can go to school with the drain in place and pin it to the inside of the shirt. If a drain is in place, the area should remain dry. If no drain is placed, the patient can shower in three days but may want to wait 5-7 days after surgery before soaking the wound.
- Medicines: Medication for pain such as acetaminophen (Tylenol®) or ibuprofen (Motrin® or Advil®) or something stronger like a narcotic may be needed to help with pain for a few days after surgery. Stool softeners and laxatives are needed to help regular stooling after surgery, especially if narcotics are still needed for pain.
- What to call the doctor for: After discharge from surgery, problems that may indicate infection such as fevers, wound redness and discharge should be addressed. If the area of surgery is swelling, bloody fluid is coming out of wound, or worsening pain occurs, call the surgeon.
- Follow-up care: The patient should be seen by a surgeon to remove the drain if one is present and to check the surgical wound.
Long-Term Outcome (“Are there future conditions to worry about?”)
Surgery is curative of this condition with excellent long term cosmetic results, resolution of pain and the ability to become more comfortable with one’s body image.
Updated: 11/2016
Author: John H.T. Waldhausen, MD
Editors: Patricia Lange, MD; Marjorie J. Arca, MD
Hepatoblastoma
Condition: Hepatoblastoma (Liver Tumor)
Overview (“What is it?”)
- Definition: Hepatoblastoma is the most common liver tumor in children and usually is diagnosed as an abdominal mass or swelling in the belly that does not cause the child pain or discomfort.
- Epidemiology: There are approximately 100 new cases of hepatoblastoma per year, or 1.6 children per million per year. A higher rate of this tumor is often found in low birth weight infants that are born prematurely. Since 1970s, the incidence of hepatoblastoma has nearly doubled for unknown reasons.
- Hepatoblastoma tumors are mostly found in children six months to three years of age.
Diagnosis (“What tests are done to find out what my child has?”)
- Labs and tests:
- Blood Tests: Several blood tests will be ordered if a liver tumor is suspected—routine labs to check for blood cell counts, liver enzyme amounts and some tumor markers such as alpha-fetoprotein (AFP).
- Imaging studies: Some or all of these studies may be performed:
- Usually when there is belly swelling, plain abdominal X-rays are obtained first. X-rays are energy beams that go through the body onto a film, making a picture on the film.
- Ultrasound uses sound waves to create images and pictures.
- Computed tomography (CT) scans: Detailed pictures of the chest or abdomen are taken, reconstructed in different views to get a better picture of the liver mass.
- MRI (Magnetic Resonance Imaging): Uses a magnet, radiowaves and computer to obtain images of organs in the body. MRI does not use radiation.
- A biopsy or taking a piece of tissue from the mass, may be needed to make a definite diagnosis by looking at the tissue under a microscope.
- Conditions that mimic this condition: Other non-cancerous liver tumors/masses such as benign hemangiomas (blood vessel abnormality) or hamartomas can mimic this tumor. Other cancerous masses that arise from the liver are hepatocellular carcinoma, germ cell tumors (infantile choriocarcinoma of the liver), undifferentiated embryonal sarcoma of the liver.
- There are several congenital (baby is already born with) conditions that are associated with hepatoblastoma such as Beckwith-Wiedemann syndrome, Trisomy 18, low birth weight infants and Familial Polyposis syndromes, to name a few.
Treatment (“What will be done to make my child better?”)
- Staging: In all types of cancer, it is important to determine if the cancer is isolated or has spread through the body. The treatment is dependent on the stage of the cancer.
- In hepatoblastoma, staging is done to look at whether the tumor can be completely removed from the liver and still leave enough liver to have function. Staging will also be done to see whether there is cancer spread in organs other than the liver.
- A pediatric oncologist (doctor that specializes in treating pediatric cancer) will guide you through the types of medicines and radiation to be used.
- Medicine: Chemotherapy are drugs that are especially aimed at destroying hepatoblastoma cells, are used either before AND after surgery or just after surgery. These are given through the vein.
- Radiation therapy may also be used if any tumor cells are left behind after surgical removal of the mass.
- Surgery: Due to the rare and complex nature of these tumors, treatment should be performed at centers/hospitals where surgeons are very familiar with hepatoblastoma. Tumors are removed if they are able to be completely resected and still leave the patient with enough liver remaining to support the patient. Occasionally, liver transplant surgeons will be involved in the decision making process as well, because transplant is sometimes the best option in certain situations.
- The mass/tumor can usually be resected at the time of diagnosis in about one-third of patients. The other two-thirds have tumors that are too large to be removed right away and will get chemotherapy first. The remaining liver will regrow and function normally.
- Preoperative preparation: Your child will require general anesthesia for any surgical procedure so he/she will have to stop eating several hours before the surgery. A shower or a bath the night prior or the day of surgery helps cleanse the skin to decrease wound infections. Certain labs may be drawn to check blood count levels and to check the function of the liver.
- Postoperative care: Your child will likely remain in the hospital for several days following the surgery in order to provide good pain control and intravenous fluids. Once he/she is eating well and able to take medications by mouth, they will be discharged.
- Central Line Placement (Port-A-Cath or Broviac Catheter) will likely be necessary to give chemotherapy drugs before or after removing the liver tumor.
- Metastases (pieces of tumor that have spread to other parts of the body, usually the lung) may require removal by surgery as well.
- Risks/Benefits:
- The main risks of surgery are bleeding and infection. Your child will likely have their blood type checked before surgery in case a blood transfusion will be necessary. They will also be given antibiotics before and maybe after surgery to help reduce the chance of infection.
- The other risk of surgery is not getting all the tumor out. This may mean that your child will need additional surgeries in the future or additional chemotherapy to rid the liver of cancer cells.
- There are risks to the drugs used to treat the tumor as well and include heart and kidney problems, lowering of blood cells, developing other tumors and the risk of infection (usually from the central line).
Home Care (“What do I need to do once my child goes home?”)
- Diet: Your child will likely be able to resume a normal diet without restrictions.
- Activity: Depending on the extent of surgery, your child might need to take it easy for a few weeks after surgery. Children tend to recover faster than adults, so they may be able to return to school and light-duty activities within a week or two.
- Wound care: Your surgeon should inform you of any specific wound care and whether or not you can get the incision wet. Call your surgeon if there is any redness or drainage from the incision or if your child has any fevers. You will also be given instructions in how to care for the central line.
- Medicines: You may be given a prescription for pain medications. Depending on the tumor, your child may need to return to the hospital or clinic to receive chemotherapy (drugs that attack cancer cells).
- In patients with cancer, especially those who are on chemotherapy, acetaminophen (Tylenol®) or ibuprofen (Motrin® or Advil®) should be avoided as fevers due to infection may be masked.
- What to call the doctor for: Call your surgeon for fevers (greater than 101° Fahrenheit), redness or drainage from the incision or for any vomiting or diarrhea.
- Follow up care: You will generally need to see your surgeon one to two weeks after your surgery and will also have a follow up with your oncology doctor.
Long-Term Outcomes (“Are there future conditions to worry about?”)
- The overall survival of babies with hepatoblastoma has been steadily improving over the last few decades. The prognosis or chance that your child will do well is dependent on success of removing the tumor and how well he/she responds to the medications.
- Your child will require long-term follow up with the oncologist as well as the surgeon to monitor for tumor coming back and for possible side effects of treating the tumor. This may involve getting your child’s blood checked periodically as well as having imaging studies performed such as CT scans or MRIs.
- If the tumor cannot be completely removed or returns after treatment, then a liver transplant may be necessary, and follow-up with a transplant surgery team may be arranged.
References:
- Pediatric Surgery; Coran, Arnold G. Copyright © 2012, 2006 by Saunders, an imprint of Elsevier Inc.
- National Cancer Institute http://www.cancer.gov/types/liver/hp/child-liver-treatment-pdq#link/_568_toc.
Updated: 11/2016
Author: Patricia Lange, MD
Editor: Marjorie J. Arca, MD
Hirschsprung Disease
Condition: Hirschsprung Disease (aganglionosis, Hirschsprung’s disease)
Overview (“What is it?”)
- Definition: Hirschsprung disease is a developmental disorder of the nerves of the intestine. The intestine contains nerves in its wall. The nerves transmit signals to the muscle of the intestinal wall that allow the intestine to move its contents forward for digestion and removal (stooling). The specific nerves of intestinal movement are called “ganglion cells”. In Hirschsprung disease, there are no ganglion cells in the wall of the affected intestine. 80-85% of children with Hirschsprung disease have the rectum and distal colon (large bowel) affected. Sometimes, a longer segment of colon, the entire colon, or even part of the small intestine may have absent ganglion cells.
- If the nerves or ganglion cells are not present in a part of the intestine, that intestine does not move things through. The affected area acts like a blockage. The baby can have a swollen belly, vomiting and inability to have stools on their own.
- Epidemiology: The incidence is about 1:5,000 children. Ganglion nerve cells are derived from special cells called neural crest cells that travel down the intestine during development. They are thought to travel from upper to lower intestinal tract. In Hirschsprung disease, this process is disturbed and the nerve stops traveling all the way down the anus. The exact reason this happens is not known.
Signs and Symptoms (“What symptoms will my child have?”)
- Early signs: Intestinal blockage in a newborn baby: 50-90% of children present during the neonatal period with a swollen belly, vomiting when feedings are attempted and no passage of stool for the first 24 hours of life.
- Enterocolitis: 10% of children with Hirschsprung disease present with an intestinal infection (enterocolitis). Since the stool is not evacuated effectively out of the body through bowel movements, bacteria multiplies in the intestines. This results in fever, abdominal swelling, diarrhea or no stools, and even spread of bacteria into the blood. Enterocolitis maybe seen in infants or older children.
- Perforation: Because the distal bowel cannot relax and decompress, the normal intestine cannot empty its contents. It becomes very distended and can rupture (perforate). There will be air and stool leaking into the abdominal cavity and this can be diagnosed on X-ray. The surgeon will recommend emergent surgery.
- Later signs/symptoms:
- Chronic constipation: Some children with Hirschsprung disease present later in childhood with chronic constipation. This is most common in breastfed infants that typically develop constipation around the time of weaning. Clinical features in older children include failure to thrive, abdominal distension and dependence on enemas, suppositories or “rectal stimulation” to pass stool. Unlike older children with behavioral associated constipation and stool holding, children with undiagnosed Hirschsprung associated constipation generally do not soil their underwear.
- Several other congenital anomalies and genetic conditions are associated with Hirschsprung Disease. These are rare, but if your child has one of these diagnoses, they may have a higher likelihood of Hirschsprung disease. These are:
- Down syndrome (trisomy 21)
- Waardenburg-Shah syndrome
- Smith-Lemli-Opitz syndrome
- Congenital hypoventilation syndrome
Diagnosis (“What tests are done to find out what my child has?”)
- The diagnosis of Hirschsprung disease is based on the clinical history, X-ray studies and a rectal biopsy.
- Plain radiographs may suggest a distal bowel blockage.
- Water-soluble contrast enema: In this study, a tube is gently placed in the rectum. Liquid dye (contrast) is injected to see if there is a narrowing of intestine (area where the nerves are not present) along with a distended intestine above the abnormal segment. This region is called where there is a difference in caliber of intestine (narrow abnormal segment and dilated normal segment) is called the “transition” zone—the transition between the narrow distal bowel with no ganglion cells and the proximal dilated colon. The study indicates approximately the length of colon without ganglion cells.
- A suction rectal biopsy is a procedure usually done at the bedside where a small instrument is inserted in the anal opening, pushed in about 2 cm and pieces of the intestinal lining is sampled (biopsy). These biopsies are sent to pathology where the presence or absence of nerves are confirmed under a microscope. In older children, a larger segment is needed (full thickness rectal biopsy). This is done under anesthesia.
- Manometry: This test is usually performed by a pediatric gastroenterologist (specialist). In this study, the relaxation of the sphincter muscle will be measured. Lack of relaxation is suggestive of Hirschsprung disease.
- Conditions that mimic Hirschsprung Disease: In infants: meconium plug syndrome, meconium ileus. In bigger kids, regular constipation can mimic Hirschsprung disease.
Treatment (“What will be done to make my child better?”)
The treatment of Hirschsprung disease is surgical, but there are a number of preoperative interventions that must be considered prior to definitive operation.
- Medical treatment: If the child has evidence of enterocolitis (infection), the first priority is fluids and antibiotics. If the baby is vomiting and/or the belly is distended, nasogastric tube is placed. Children with enterocolitis or those in whom immediate surgery cannot be done for other reasons should undergo bowel decompression by rectal irrigations, removing the stool and bacteria from the intestine.
- Surgery: The timing of the definitive surgery for Hirschsprung differs in certain situations. In some centers, definitive surgery is performed in a baby once the diagnosis is made. In other centers, definitive surgery is postponed until the baby is bigger. In this case, the baby goes home on rectal irrigations in order to evacuate stool.
- Stoma: A temporary stoma may be necessary in certain situations. A stoma is a surgery that sews the end of the colon to the abdominal wall so that a bag can be applied for the stool to drain. For children with severe enterocolitis, perforation (a hole in the bowel from high pressure), poor nutrition, or an older child with extensively dilated proximal bowel, a temporary stoma may be recommended.
- Pull-through procedures: A “pull-through procedure” is the definitive procedure for HD. The main goals of this procedure are to remove the abnormal segment of bowel that has no nerves and connect the normally innervated segment of intestine to the anus. There are several operations to accomplish these goals (names are Soave, Swenson and Duhamel). Which type of pull-through is best for your child depends on many factors and will be discussed by your surgeon. The pull-through procedures can be done using open on minimally invasive (laparoscopic) approach.
- Laparoscopic surgery: In laparoscopic surgery, several small cuts (incisions) are made. Through one of the cuts, a video camera is placed. The surgery itself is done using small instruments placed through the other incisions. The usual number of incisions (cuts) for laparoscopic surgery vary.
- Open surgery (laparotomy) uses larger incision, either vertical or transverse to perform the operation.
- Long-segment disease: This is usually defined as lack of ganglion cells to the mid-transverse colon area (half the large bowel). At times the entire colon can be involved. There is often a positive family history. The surgeon may suspect long-segment disease from the appearance of the contrast enema. The rectal biopsy will have absent ganglion cells, but may also have other subtle differences.
- Once the level of ganglion cells is determined, most surgeons create a stoma, wait for complete pathology reports and plan reconstruction at a later date.
- The surgeon will discuss the details of the particular pull-through recommended, based on their experience. For total colonic involvement, a straight pull-through is frequently done. Although stool output may be high at first, this will decrease over time.
- Risks of surgery: The surgeon will observe for the following possible complications:
- Wound infection
- Bleeding
- Anastomotic leak: The rectal sutures leak and cause infection
- Stricture (scarred narrowing of the rectal suture line)
- Bowel obstruction: Can be due to an adhesion, a twist in the pull-through or the rectal cuff where the bowel is pulled through can scar tightly and cause a blockage. The child will have a distended abdomen and vomiting.
- Fistulas: Connections between bowel and bladder or bowel and vagina have been reported to develop after operation. These are rare problems.
- Benefits of surgery: Ability to evacuate stool normally.
- Near Total Intestinal Aganglionosis: Rarely, almost the entire intestinal tract has no ganglion cells, leaving only 10-40 cm of normally innervated small bowel. In most of these cases, there is not enough functional small bowel to support nutrition and growth. These children must be fed from birth through the vein with total parenteral nutrition. The surgeon may recommend a stoma in the area where there are ganglion cells. These children are considered to have intestinal failure. They require detailed care from physicians, usually pediatric gastroenterologists, with experience caring for intestinal failure patients.
- Older children: Children diagnosed later in childhood may have an extensively dilated colon. Usually the dilated portion is removed, the level of ganglion cells is determined, a temporary stoma is done. This allows the dilated bowel to shrink. A pull-through operation is planned for a later date when the bowel is more decompressed.
- Preoperative preparation: If the operation is scheduled (elective), a bath or shower is recommended the night before or the morning prior to surgery. The child will not eat anything for 6-8 hrs before surgery. Intravenous antibiotics will be given in the operating room.
- Postoperative care: Once the child has stool out of the bottom or stoma, diet is resumed. Activity is normal. Medications for pain will be given.
Home Care (“What do I need to do once my child goes home?”)
- Diet: Your child may eat a normal diet after surgery.
- Activity: Your child should avoid strenuous activity and heavy lifting for the first week after laparoscopic surgery, 4-6 weeks after open surgery.
- Wound care: Surgical incisions should be kept clean and dry for a few days after surgery. Most of the time, the stitches used in children are absorbable and do not require removal. Your surgeon will give you specific guidance regarding wound care, including when your child can shower or bathe.
- Medicines: Medicines for pain such as acetaminophen (Tylenol®) or ibuprofen (Motrin® or Advil®) or something stronger like a narcotic may be needed to help with pain for a few days after surgery. Stool softeners and laxatives are needed to help regular stooling after surgery, especially if narcotics are still needed for pain.
- What to call the doctor for: Call your doctor for worsening belly pain, fever, vomiting, diarrhea, problems with urination or if the wounds are red or draining fluid.
- Follow-up care: Your child should follow up with his or her surgeon 2-3 weeks after surgery to ensure proper postoperative healing.
- The surgeon will check the anastomosis (rectal stitches) at about two weeks after the pull-through. Some surgeons teach the parents how to dilate the anastomosis so it does not become narrow.
- Barrier cream: This is needed for some time, as diaper rash can be severe.
- Enterocolitis (see above)
- Back pressure on a colonic biopsy site can cause it to perforate.
Long-Term Outcomes (“Are there future conditions to worry about?”)
- Occasional problems related to the bowel are fairly common in the first few years of life. The surgeon will follow the child until after the toilet training process, longer if needed.
- Ongoing obstructive symptoms: There are a range of obstructive symptoms that can occur after a pull-through.
- Mechanical obstruction
- Stricture: If the anastomosis scar tightens and narrows, sometimes it can be dilated. Surgery may be needed.
- Twist: If a twist in the pull-through is identified, surgery will be needed to correct it.
- Persistent aganglionosis: This is usually due to a pathologist error or lack of blood flow/inflammation of previously normal bowel causing nerves to die. A repeat biopsy may show that the pull-through was performed in an area without ganglion cells. Surgery will be needed to place the pull-through at the correct level.
- Motility Disorder: Children with Hirschsprung disease have a higher incidence of dyscoordination of the propulsive waves through the bowel (motility disorder) despite no obstruction, and normal ganglion cells in the rectum after pull-through operation. They may benefit from evaluation by a pediatric gastroenterologist and recommendations for bowel management.
- Internal sphincter achalasia: All children with Hirschsprung disease have an absent rectal inhibitory reflex, (the sphincter may not relax normally), but it is unclear why some develop obstructive symptoms from this and some do not. Sometimes the sphincter is tight, the bowel dilates and the patient has obstructive symptoms. Most outgrow the problem by age five years. The surgeon may recommend Botox injection of the sphincter. Botox relaxes the sphincter, but is only good for a few months. This diagnoses and treats the problem, and is generally successful.
- Functional megacolon: Stool-holding behavior is a common cause of constipation after pull-through operation. Passing hard, painful stools can start a cycle of withholding behavior. A bowel management program may be recommended.
- Soiling: The surgeon may recommend investigations to have a clear understanding of the cause of the soiling. Physical exam including rectal exam, X-rays, contrast enema and manometry may be recommended. The surgeon will determine the intactness of the sphincter and degree of normal rectal sensation. A treatment plan will be developed based on whether the soiling is due to a sphincter problem or rectal sensation problem, slow transit through the bowel with overflow of stool, stool holding behavior with overflow, or hyperperistalsis (rapid transit of stool due to abnormal motility).
- Enterocolitis: Enterocolitis may present both before and after surgical correction of Hirschsprung disease. It may present in children after operation who never had it preoperatively. It is the most common cause of death in children with Hirschsprung disease. It is more common in younger children, those with long segment disease and children with Down’s syndrome. The symptoms include fever, distension and diarrhea. X-ray abnormalities are present. Treatment involves nasogastric drainage, antibiotics, intravenous fluids and decompression of the colon and rectum, usually by irrigations. Enterocolitis can be minimized by the routine use of irrigations. Some surgeons also prescribe a regular dose of an antibiotic. If any of the above symptoms occur, the surgeon or a physician should be contacted immediately.
- Mechanical obstruction
- Resolution over first five years: Obstructive symptoms, soiling and enterocolitis (in the absence of obstruction), usually resolve in the first five years of life. Studies of teenagers suggest social satisfaction and quality of life normalize by the late teen years.
- Ongoing incontinence, enterocolitis and dehydration are more common in children with long-segment disease, Down’s syndrome or other causes of neurological impairment. Their long-term results are less satisfactory.
Updated: 11/2016
Author: Patricia Lange, MD
Editor: Marjorie J. Arca, MD
Hyperthyroidism
Condition: Hyperthyroidism (also known as Grave’s disease)
Overview (“What is it?”)
- Hyperthyroidism is a condition when the thyroid gland in the neck becomes overactive and produces too much thyroid hormone. The thyroid is a gland in the neck that makes hormones that help the body grow. Any imbalance in hormone production affects the body in a negative way. Thyroid hormone stimulates the body’s metabolism, so too much thyroid hormone causes the body to work abnormally hard.
- Epidemiology: Conditions that affect the thyroid are not common in children and can occur in about 37 out of 1,000 children. The most common conditions include generalized enlargement of the thyroid (also called goiter or thyroiditis). Thyroiditis can come about due to several reasons. One reason can be that certain medications that one might be taking for a separate reason cause the thyroid to become larger. Other reasons for thyroiditis include an inflammatory or an autoimmune condition (one example is Graves’ Disease also called diffuse toxic goiter) that can occur which leads to thyroid enlargement. The thyroid can also be enlarged due to many cysts within the thyroid gland that are normally not supposed to be in the gland. A virus can even cause the thyroid gland to be enlarged and painful. Lastly, not having enough iodine from diet sources can cause the thyroid to be enlarged. In other parts of the world, this can be the most common reason for having an abnormally enlarged thyroid.
- Thyroid nodules (one or more separate masses in an otherwise normal sized thyroid gland) are even more uncommon in children than the condition above where the whole thyroid gland is enlarged. However, thyroid nodules in children can be cancerous 20% of the time. The most common reason why a person would have a cancerous thyroid nodule would be history of neck irradiation.
Signs and Symptoms (“What symptoms will my child have?”)
- Early signs: Childhood symptoms include nervousness, irritability, diarrhea, weight loss, insomnia, fatigue, hair thinning and poor performance in school. On examination they may have high blood pressure, fast heart rate and weight loss.
- Later signs/symptoms: Neck swelling (goiter) and exophthalmos (protruding eyes), weight loss, sweating, heart palpitations (irregular heart beat) may be seen over time.
Diagnosis (“What tests are done to find out what my child has?”)
- Labs and tests: Blood is checked for increased levels of thyroid hormones (T4 and T3). TSH, a hormone from a gland in the brain (pituitary gland) which stimulates the thyroid, should be low unless there is a pituitary tumor present.
- A thyroid scan may also demonstrate increased uptake (activity) throughout the gland. In this test, a very small amount of radioactive iodine tracer is injected in the vein and followed by a body detector to see how much is taken up by the thyroid gland.
- An ultrasound of the thyroid gland may be obtained if there is a question of a mass or a lump in the gland. An ultrasound uses sound waves to create an image or picture of parts of the body without using radiation.
- Obtaining thyroid tissue by using a needle inserted into a thyroid nodule—also called fine-needle aspiration (FNA)—may give information about thyroid nodule (not thryroiditis) and guide the next step in management. Ultrasound can guide the surgeon to where the needle can be placed to target the nodule.
- Conditions that mimic this condition: An enlarged thyroid gland can sometimes be caused by thyroid cysts, tumors or inflammatory conditions of the thyroid (thyroiditis).
Treatment (“What will be done to make my child better?”)
- Medicine: Depending on the kind of thyroiditis a child has, anti-inflammatory medicines, steroids or antibiotics and time is needed for the condition to get better. It can take two months to more than a year for some therapies for the child to get well fully. For Graves’ disease, anti-thyroid medication that block thyroid hormone production are usually tried first. These are quite effective. Sometimes, medication that blocks the side effects of racing heart rate and high blood pressure are added (beta blockers). Long-term remission may be achieved in 25-65% of patients after the medications are stopped.
- Radioactive isotopes: This method of treatment uses highly radioactive iodine (radioactive I131) to destroy the thyroid gland. The radioactive iodine is given through a vein, and it is taken up by the thyroid gland. The radioactivity destroys the thyroid. This is a good approach in some patients who are not good candidates for medical therapy or surgery. Although effective, there is concern that the long-term incidence of hypothyroidism (low thyroid levels) is increased especially when used in children. Typically, radioactive iodine is not recommended in kids younger than five years of age.
- Surgery: Surgery is reserved in thyroiditis for patients who do not respond to medicines, unable to get radioactive iodine. Total or near-total thyroidectomy (removal of all or part of the thyroid gland) is needed. Depending on the extent of the operation and the size of the gland removed, a drain may be left in place to gather fluid that may collect post-operatively
- Preoperative preparation: Patients are often started on a hormone blockade and a beta blocker preoperatively, to protect against the release of extra thyroid hormone during the operation. Extra release of hormones may increase the heart rate and blood pressure at dangerously high levels during the stress of surgery.
- Postoperative care: An overnight stay is usually recommended. Pain medications are given. Blood levels of calcium may be monitored as well as quality of voice (hoarseness or breathiness).
- Risks/Benefits: Surgery is very effective in treating hyperthyroidism. However, it does require an operation with complications occurring roughly 5% of the time. Complications include bleeding, wound infection, damage to the nerves that control the vocal cords, damage to the glands that control calcium levels in the blood. Of these complications, 1-2% may persist long term.
Home Care (“What do I need to do once my child goes home?”)
- Diet: Normal
- Activity: Normal
- Wound care: Keep the incision clean and dry for about three days after surgery. The child may shower after three days, but do not soak the wound for about a week.
- Medicines: Medication for pain such as acetaminophen (Tylenol®) or ibuprofen (Motrin® or Advil®) or something stronger like a narcotic may be needed to help with pain for a few days after surgery. Stool softeners and laxatives are needed to help regular stooling after surgery, especially if narcotics are still needed for pain.
- Take any thyroid hormone replacements as directed.
- If calcium levels are found to be low, calcium supplements may be necessary.
- What to call the doctor for: Wound redness, swelling or drainage, recurrence of symptoms (racing heart rate, palpitations), changes in voice patterns, tingling and numbness of the fingers and around the mouth.
- Follow-up care: You will follow up with your surgeon to check the wound and make sure things are healing well. Your pediatrician and/or endocrinologist will check thyroid hormone levels to make sure that these normalize after surgery.
Long-Term Outcomes (“Are there future conditions to worry about?”)
- The two major long-term risks of surgery are hoarseness caused by injury to the nerve that controls the voice box that runs adjacent to the thyroid gland and low calcium levels due to injury to the glands (parathyroid) that control calcium.
- If medications are used initially to treat the enlarged or overactive gland and the thyroid continues to cause symptoms, then surgery may be necessary.
- Your child will likely require long-term follow up with his/her pediatrician or endocrinologist (doctor specializing in disorders of endocrine glands such as the thyroid gland).
Updated: 11/2016
Author: Kathryn Q. Bernabe, MD; Michael B. Ishitani
Editors: Patricia Lange, MD; Marjorie J. Arca, MD
Hypertrophic Pyloric Stenosis
Condition: Hypertrophic Pyloric Stenosis (HPS)
Overview (“What is it?”)
- Hypertrophic pyloric stenosis (HPS) is a narrowing of the pylorus muscle. The pylorus is a sphincter muscle along the end of the stomach that controls the passage of food into the small intestine. (See Figure 1.)
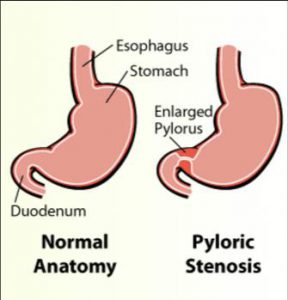 Figure 1
Figure 1
- When the sphincter becomes hypertrophied (thicker than normal), the opening of the pylorus becomes too narrow for food or liquids to pass through. This leads to excessive nonbilious (not green), projectile (“shooting out”) vomiting.
- Hypertrophic pyloric stenosis is a relatively common condition that occurs more commonly in first-born male infants. It is believed to occur in approximately 1 in 300 to 900 live births.
- There is no known cause of HPS.
- It appears to occur more frequently in males and may happen more often in the same family. However, most infants have no family history of HPS.
Signs and Symptoms (“What symptoms will my child have?”)
- HPS is usually diagnosed between two to eight weeks of life. The most common symptom that is observed is worsening vomiting.
- Projectile, (or forceful shooting) vomiting is the hallmark of HPS. The vomited fluid consists of formula. The vomiting may be intermittent at first, but will start to occur more often and can become projectile in nature.
- Your infant may continue to be hungry even after vomiting.
- If vomiting continues over days, the baby can be dehydrated. The baby may not urinate as often and may not have tears when crying.
- Blood levels of electrolytes (minerals such as sodium, bicarbonate and potassium) in the blood can be abnormal because of losses during vomiting.
Diagnosis (“What tests are done to find out what my child has?”)
- HPS may be diagnosed by physical exam where the pylorus can be felt by pressing on the abdomen.
- Most times an ultrasound will be performed to diagnose HPS. Ultrasound uses sound waves to create images of the pylorus which is seen to be longer and thicker than normal and does not allow liquid in the stomach to go through.
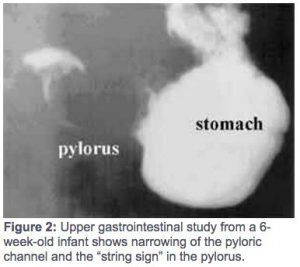 Less commonly, a radiological test called an upper gastrointestinal contrast study may be performed. The baby takes a liquid that lights up on X-ray. X-ray pictures of the stomach is taken. In HPS, only a very small amount of contrast gets out of the stomach. (See Figure 2)
Less commonly, a radiological test called an upper gastrointestinal contrast study may be performed. The baby takes a liquid that lights up on X-ray. X-ray pictures of the stomach is taken. In HPS, only a very small amount of contrast gets out of the stomach. (See Figure 2)
Treatment (“What will be done to make my child better?”)
- The treatment for HPS is a surgical procedure called a “pyloromyotomy”. The goal of the surgery is to make a cut in the thickened pylorus muscle and open the passage between the stomach and the small intestine. The surgery may be done laparoscopically or open.
- Laparoscopic pyloromyotomy: Several small cuts (incisions) are made. Through one of the cuts, a video camera is placed. The surgery itself is done using small instruments placed through the other incisions. Sometimes the surgery cannot be performed laparoscopically.
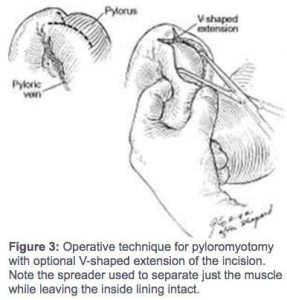 Open pyloromyotomy (Figure 3): A cut is made usually in the right upper part of the belly or around the belly button. The pyloromyotomy involves making a cut through the thickened pyloric muscle while leaving the inside layer intact. This will allow food to pass through the pylorus and into the small intestine.
Open pyloromyotomy (Figure 3): A cut is made usually in the right upper part of the belly or around the belly button. The pyloromyotomy involves making a cut through the thickened pyloric muscle while leaving the inside layer intact. This will allow food to pass through the pylorus and into the small intestine.- Risks of undergoing surgery include, but are not limited to: the risks of anesthesia, bleeding, infection and unintended damage to other structures in the body. The inside lining of the stomach may also be cut during the pyloromyotomy. This will be repaired and it may take a longer to start feeding the baby in order to allow the area to seal. An additional risk of the surgery is that an inadequate incision is made in the pylorus muscle. This is rare and a second surgery may be required to correct this.
- Benefits: The stomach will be able to empty food into the small intestine, and the baby will be able to eat without vomiting.
- Preoperative preparation: Before surgery can be performed, the infant must be given additional fluids to improve the dehydration and correct abnormalities of the electrolyte (mineral) levels in the blood stream. Correcting these problems will make the baby better tolerate surgery and anesthesia better.
- Postoperative care: The baby will be allowed a few hours to recover from anesthesia and allowed to drink at the discretion of the surgeon. For pain, the baby is given acetaminophen (Tylenol®).
Home Care (“What do I need to do once my child goes home?”)
- Vomiting may still occur initially after surgery, but will usually resolve.
- Feeding is typically started around 4-6 hours after the surgery. Your surgeon will discuss the feeding plan after surgery.
- If all goes well, your infant will be discharged within one day of surgery.
- Surgical incisions should be kept clean and dry for three days after surgery. Afterwards, the wounds may be washed with soap and water but not soaked for about seven days after surgery. Most of the time, the stitches used in children are absorbable and do not require removal.
- Follow-up: You will follow up with the pediatric surgeon afterwards to make sure your infant is eating well, gaining weight and healing incisions.
- When to call your doctor: Redness or drainage of the wound, fevers, vomiting often, swelling of the belly.
Long-Term Outcomes (“Are there future conditions to worry about?”)
Long-term outcomes are excellent with a very low rate of complications.
References:
- Chung, Dai. “Pediatric Surgery.” Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice. 19th ed. Saunders, 2012. 1821-1871. Print.
- Hackham, David J., Tracy C. Grikscheit, Kasper S. Wang, Kurt D. Newman, and Henri R. Ford. “Pediatric Surgery.” Schwartz’s Principles of Surgery. 9th ed. McGraw-Hill. 2012. 1409-1447. Print.
- Sato, Thomas T., Oldham, Keith T. “Pediatric Abdomen.” Greenfield’s Surgery: Scientific Principles & Practice. 5th ed. Lippincott Williams & Wilkins. 2010. Print.
Updated: 11/2016
Author: Romeo C. Ignacio, Jr., MD: A. Kastl, MD
Editors: Patricia Lange, MD; Marjorie J. Arca, MD
Inguinal Hernia/Hydrocele
Condition: Inguinal Hernia/Hydrocele
An inguinal hernia happens near the groin area, between the belly and the thigh. With boys you can often see a swelling in the scrotom. Does this mean girls are off the hook? Not exactly. Although girls don’t have testicles, they do have an inguinal canal and can get hernias too. About 3-5% of healthy, full-term babies are born with an inguinal hernia. In premature infants, the incidence is substantially increased – up to 30%!
If an inguinal hernia is not treated, it can cause serious problems. Learn more about the signs and symptoms of this condition and what to expect if your child needs hernia repair surgery.
The source of this content is the American Academy of Pediatrics Section on Surgery, APSA and the American College of Surgeons. Copyright 2019.
Intussusception
Condition: Intussusception
Overview (“What is it?”)
- Intussusception [in-tuh s-suh-sep-shuh n] is the condition when part of the intestine slides into an adjacent part of the intestine. It is similar to the intestine telescoping into itself. When the intestine telescopes into itself, this portion of the intestine (intussusception) gets kinked. This then leads to the cut off of the blood supply to that part of the intestine and blocks the passage of food and fluid.
- Intussusception occurs more frequently in males. Although intussusception can occur in all pediatric ages, 75% of cases occur in the first two years of life and 90% in children by three years old. There is a seasonal variation that correlates with viral infections where most occur during May to July.
 Figure 1.
Figure 1.
Signs and Symptoms (“What symptoms will my child have?”)
- Early signs/symptoms: (1) intermittent episodes of sudden onset of severe abdominal pain that lasts only a few minutes. Infants may pull up their legs during episodes of pain; (2) vomiting; (3) abdominal mass in the right upper side of the abdomen; (4) lethargy due to dehydration.
- Later signs/symptoms: (1) bloody stools with a mucus-like texture that resemble currant jelly; (2) bilious (green) vomiting from intestinal obstruction; (3) fever, low blood pressure, and fast heart rate can be signs of bowel perforation.
Diagnosis (“What tests are done to find out what my child has?”)
- Labs and tests: The most common blood tests obtained are complete blood count (CBC) and electrolytes. The white blood cell count may be high if the intussuscepted bowel is compromised or ischemic (lack of blood flow). The most accurate initial study is ultrasound. Ultrasound may show concentric rings of affected intestine and is termed a “target sign”. A contrast enema (injecting dye or air into the colon) may be both diagnostic and therapeutic.
- Conditions that mimic this condition: Include other causes for bowel obstruction such as malrotation and midgut volvulus. Conditions that cause cramping pain such as gastroenteritis may also mimic intussusception.
Treatment (“What will be done to make my child better?”)
- Medicine: The initial treatment for patients with intussusception is fluid resuscitation as most patients are dehydrated. If the patient is stable, radiologic reduction is attempted with liquid or air contrast enemas under fluoroscopic or sonographic guidance. This can usually be attempted multiple times. If radiologic reduction is successful, the radiologist will see a sudden rush of air or barium flow into the distal ileum. After successful enema reduction, the child is typically admitted to the hospital for observation to watch for recurrence. In some instances, patients can be discharged from the Emergency Room once they tolerate fluids and are relieved of pain and other symptoms.
- Surgery:
- Preoperative preparation: Surgery is indicated for patients with suspected ischemic or compromised bowel. These patients may have free air on X-rays or evidence of worsening infection (sepsis) and tenderness (on physical exam). Other reasons for surgery include suspicion of a pathologic lead point such as a diverticlum or polyp, or failed attempts from radiologic reduction. The type of intervention will be individualized and discussed by the treating team. Patients will be started on antibiotics and may need transfusions of blood products prior to surgery.
- Postoperative care: Patients will not be fed for a period of time after surgery until their intestine begins to work again. Patients may require additional procedures.
- Risks/Benefits: In the majority of patients, reduction of the intussusception is successful with contrast enema and surgery is avoided. There is a small risk of the intestine being injured during the contrast enema necessitating surgery. If patients are clinically deteriorating or have free air on X-ray, surgical intervention is required. Sometimes, part of the intestine may need to be removed.
Home Care (“What do I need to do once my child goes home?”)
- Diet: Regular diet.
- Activity: Normal pediatric activity.
- Wound care: None
- Medicines: None
- What to call the doctor for: Monitor for recurrent symptoms that include abdominal pain, vomiting, bloody stools.
- Follow-up care: If patient had surgery, follow up in 1-2 weeks. If patient had radiologic reduction, routine follow-up with pediatrician.
Long-Term Outcomes (“Are there future conditions to worry about?”)
There are usually no long-term complications. However, on average, there is roughly a 5% recurrence rate after radiologic enema reduction. Recurrence usually occurs within 6 months of the original episode. If patient had surgery, a potential condition is the development of scar tissue within the abdomen (adhesions) that can lead to bowel obstructions. After surgical reduction of the intussusception, there is also a 5% chance the intussusception can recur.
Updated: 11/2016
Authors: Steven L. Lee, MD; Nhan Huynh
Editors: Patricia Lange, MD; Marjorie J. Arca, MD
Labial Adhesions
Condition: Labial Adhesions (labial fusion or labial agglutination)
Overview (“What is it?”)
- A condition in young girls where the inner lips of the vagina—called labia minora—have become stuck together. The affected area that is joined or stuck may be just a small section, or it may be the entire length of the vagina.
- Occurs in about two percent of young girls (between the ages of three months to six years) in the United States.
- Once girls begin puberty, a hormone called estrogen increases in their blood stream, these adhesions are less common or may separate on their own.
- Other possible causes of labial adhesions are chronic inflammation from fecal soiling, vulvovaginitis (inflammation around the area of the vagina), eczema or dermatitis (skin inflammation) from soaps or detergents.
Signs and Symptoms (“What symptoms will my child have?”)
- Most children will have no symptoms or problems. No treatment is required.
- However, common symptoms or complaints can include:
- Urinary dribbling which is due to urine that gets trapped behind the adhesion or fused labia, later dribbling out.
- Skin or vaginal irritation or redness.
- Frequent urinary tract infections as a result of the adhesions.
Diagnosis (“What tests are done to find out what my child has?”)
- This condition can be easily diagnosed by physical exam. A doctor or health care provider can evaluate your child for this condition.
- If your child has symptoms or problems, go seek medical evaluation by a doctor who will evaluate the area.
Treatment (“What will be done to make my child better?”)
- In most cases, where the child is having no problems, nothing needs to be done. Do not attempt to separate the adhesions at home because they can hurt and tend to recur or scar again.
- Medical Treatment: Children with problems can be initially treated with an estrogen cream. A doctor will prescribe the medication and tell you to apply this cream directly to the affected tissue, and in about two weeks—sometimes more, sometimes less—the labia should separate.
- Apply the cream with a cotton swab to the fusion line, and try not to get much on the surrounding tissues. Some doctors suggest switching to a nonprescription lubricating ointment like petroleum jelly or baby salve after you stop using the estrogen cream, to reduce risk of recurrence of adhesions.
- Surgery: If medical care does not result in separation of the labia minora or if urinary retention or UTIs are present, manual or surgical separation (also known as lysing) may be considered.
- Lysing (breaking down) the adhesions is needed if the adhesions are causing symptoms. Manually breaking down the adhesions in the doctor’s office, after applying a topical anesthetic cream, may be another option for treatment. If your doctor recommends, this can also take place under a short general anesthesia in the operating room if the adhesions are very thick. In either situation, it will be important to apply Vaseline® to either side of the labia so it does not reattach as it heals.
- Preoperative preparation: The child should bathe or shower the night before or the morning of surgery. She should not eat anything solid eight hours before surgery and 2-4 hours for liquid. Ask your surgeon’s office regarding when to hold feeding for your child.
- Postoperative care: Once the labial adhesions have been separated, either by medical means or through surgical, an ointment (examples: antibiotic ointment or diaper rash cream) should be applied several times a day for several months to allow the labial edges to heal without repeat adhesion formation.
Prevention
- While your child is in diapers, be vigilant about making sure the diaper is dry.
- Avoid scented soaps or detergent that may cause irritation, too.
Long-Term Outcomes (“Are there future conditions to worry about?”)
- While your child is using the estrogen cream, it is important to watch for known side effects (development of pubic hair, breast budding, general irritation). Once the cream is stopped, the side effects may go away.
- Because labial adhesions are usually asymptomatic and rarely constitute an emergency, follow-up care should be provided in the doctor’s office.
Updated: 11/2016
Author: Romeo C. Ignacio, Jr., MD
Editors: Patricia Lange, MD; Marjorie J. Arca, MD
Malrotation
Condition: Malrotation (rotational anomalies, malrotation with volvulus)
Overview (“What is it?”)
- Malrotation is the failure of normal intestinal rotation and fixation during the development of the fetus. In the first trimester of pregnancy, the lungs develop very quickly and the fetus’ (baby’s) intestines go outside of the belly for a certain time then returns back to the belly. Malrotation happens when the intestine does not follow the normal way that they are supposed to be inside the belly. When malrotation is present, there are two things that can give a child problems: (1) volvulus which is when the intestine twists upon itself, cutting off its own blood supply and (2) abnormal adhesions or bands that can partially block the passage of contents within the intestines. Volvulus (Figure 1) is dangerous because it can cut off the blood supply to most of the intestines causing the intestines, and sometimes the child, to die.
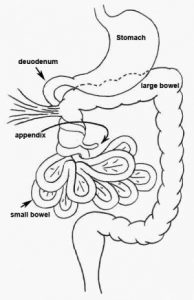 Figure 1. Volvulus
Figure 1. Volvulus
- Malrotation occurs in 1 in 200 to 500 of live births. Most patients are asymptomatic. Symptomatic malrotation occurs in approximately 1 in 6,000 of live births. Most patients have problems in the first months of life.
Signs and Symptoms (“What symptoms will my child have?”)
- Early signs of malrotation depend of the problems it is causing. If there are abnormal bands that are partially blocking the intestines, the baby may have intermittent vomiting that may interfere with weight gain. If there is volvulus, the classic symptom is bilious (green or bright yellow) vomiting.
- Later signs/symptoms of malrotation with volvulus include firm, distended and painful belly. There may also be blood in the stool and shock. These symptoms may signal dead intestine.
Diagnosis (“What tests are done to find out what my child has?”)
- Labs and tests: If the baby has lots of vomiting, blood tests will be sent to check levels of electrolytes (minerals) in the blood.
- Imaging studies:
- Abdominal X-rays may be obtained in a child with vomiting, initially to look for causes of vomiting.
- An upper gastrointestinal contrast study is the test of choice if malrotation is suspected. In this study, the child is given contrast to drink. Several X-rays are taken to follow the course of the contrast through the stomach and the intestine. This study would show whether the positioning of the intestines is normal or not.
- An ultrasound may be helpful to look for other causes of vomiting and belly pain such as intussusception.
- Conditions that mimic this condition include intestinal atresia, annular pancreas, meconium ileus, intussusception, Hirschsprung disease, gastroesophageal reflux, gastroenteritis.
Treatment (“What will be done to make my child better?”)
- Treatment for malrotation depends on the symptoms that the child has, the overall health, and the degree of malrotation. For example, in children with complex cardiac problems and malrotation but with NO symptoms related to malrotation, surgical intervention is not recommended. In these children, there is high risks for surgery but potentially little benefit. In children who has symptoms of vomiting and inability to gain good weight or to advice volume of feeding, doing surgical repair is done on a scheduled basis. In patients with volvulus where the blood supply to the intestine is potentially cut off, the repair is done on an emergency basis. In these cases, the longer the intestines don’t have blood flow, the higher risk it is for the intestines to die.
- Malrotation without volvulus
- Medicine: No medicine can make this condition better.
- Surgery: This is usually a scheduled operation. The name of the procedure for malrotation is called “Ladd’s procedure”—named after the surgeon who invented it. The abnormal bands causing partial obstruction are released, the integrity of the blood supply to the intestines is reassured and the appendix is removed. In malrotation, the appendix is not in the normal position, and this is why it is removed. In this set of patients, Ladd’s procedure can be done the traditional way (“open” or larger incision) or laparoscopic.
- Open: Ladd’s procedure is done through a transverse cut in the right upper part of the belly or through a vertical cut in the middle of the belly.
- Laparoscopy: Several small cuts (incisions) are made. Through one of the cuts, a video camera is placed. The surgery itself is done using small instruments placed through the other incisions. The usual number of incisions (cuts) for laparoscopic surgery vary from one (single port umbilical) to multiple.
- Preoperative preparation: Your child should shower or bathe the night before or the morning of surgery. Prior to surgery, antibiotics may be given through the vein.
- Postoperative care:
- Activity: Typically, the child is encouraged to resume regular activity as soon as possible.
- Diet: Oral feeding will resume once there is evidence that the intestines have recovered from surgery. This is different from patient to patient.
- Medicines: Your child may need any of the following:
- Antibiotics: To help prevent or treat an infection caused by bacteria.
- Anti-nausea medicine: To control vomiting (throwing up).
- Pain medicine: Pain medicine can include acetaminophen (Tylenol®), ibuprofen (Motrin®), or narcotics. These medicines can be given by vein or by mouth.
- Malrotation with volvulus
- Medicine: Patients with malrotation with midgut volvulus will need an IV for fluids and medicines to fight infection (antibiotics). If the patient is in pain, medications to help relieve discomfort may be needed.
- Surgery: Volvulus is a surgical emergency! The procedure is usually done through a horizontal or vertical cut in the belly. First, the intestines are untwisted to restore blood flow. The intestines are assessed to see how much damage is there. Sometimes, untwisting and restoring blood flow revives intestine. If the intestines are damaged beyond repair, then they will need to be removed. After the damage to the intestines are assessed and taken care of, then a Ladd’s procedure is performed.
- Preoperative preparation: Patients need to be given fluids and antibiotics through the vein. Transfusions of blood products may be needed.
- Postoperative care: Patients will remain on antibiotics after surgery. Patients will not be fed for a period of time after surgery until their intestine begins working again. If there is a question on whether segments of intestine can recover, repeated examinations under anesthesia may be required prior to final closure.
- Risks/Benefits:
- Risks of abdominal surgery include bleeding, infection, injury to abdominal structures.
- Benefits: Surgical intervention is required to deal with complications of malrotation with or without volvulus. In cases where there is suspected volvulus, surgery may be lifesaving.
Home Care (“What do I need to do once my child goes home?”)
- Diet: Will be based on how much intestine is remaining.
- Activity: Normal infant/pediatric activity
- Wound care: None
- Medicines: Usually none
- What to call the doctor for: Green vomit, not tolerating feedings, fever or signs of a wound infection (redness or drainage).
- Follow-up care: Surgery follow-up in 1-2 weeks. Routine pediatrician follow-up.
Long-Term Outcomes (“Are there future conditions to worry about?”)
- For malrotation without volvulus, long-term outcomes are excellent. There is a 10-15% risk of intestinal obstruction in the child’s lifetime. This complication is usually suspected if green or bright yellow vomiting, belly pain happens.
- Long-term outcomes in patients with volvulus where intestines needed to be removed are dependent upon the length of intestines remaining after surgery. Children with no bowel removed or very little removed will have normal intestinal function. Those with a lot of small bowel removed may be unable to sustain their nutrition by intestinal feeding alone and require nutrition given through the veins. Very close follow up with surgery and gastroenterology (specialists of intestinal function) is needed.
Updated: 11/2016
Authors: Steven L. Lee, MD; Nhan Huynh
Editors: Patricia Lange, MD; Marjorie J. Arca, MD
Meckel's Diverticulum
Condition: Meckel’s Diverticulum
Overview (“What is it?”)
- A Meckel’s Diverticulum (MD) is a condition where there is a congenital (baby was born with it) extension of the small intestine. It is a remnant of a normal structure (vitelline duct) that is present in all babies as they develop inside their mothers. This structure usually disappears completely before the baby is born.
- Meckel’s Diverticula affects about 2% of the population, but most of the time, they do not cause symptoms.
- Meckel’s Diverticula are also known as ‘the great mimickers’ because they can masquerade as many other problems.
Signs and Symptoms (“What symptoms will my child have?”)
- Symptoms arising from Meckel’s Diverticulum can vary. They can present at any age.
- Bleeding: Some MD possess stomach tissue within it. Stomach tissue makes acid causing an ulcer which can bleed or result in a hole (perforation). The amount of bleeding from MD can be pretty massive. There is frankly bloody stools without associated abdominal pain. If the blood loss is severe, there may be sleepiness or shock.
- Infection: MD can be infected. The pain is usually in the lower abdomen. There may be fever.
- Obstruction: MD and its attachments can be a focal point for intestine to twist around. Nausea and vomiting may be present.
- Perforation: A hole can result in a MD from an inflammatory process. Fever and abdominal pain may be seen.
Diagnosis (“What tests are done to find out what my child has?”)
- Labs and tests: Blood count (CBC) will be checked if the child has bleeding. In a vomiting child, levels of minerals (electrolytes) will be checked to see how bad the dehydration is.
- Imaging
- Bleeding:
- A Technetium 99m pertechnetate nuclear medicine scan can show whether someone has MD. In this test, a small amount of radioactive material is injected in the vein. It is taken up by MD if stomach tissue is present in MD. Occasionally, the nuclear scan does not perfectly visualize the gastric tissue.
- Tagged RBC scans may pinpoint the source of bleeding, but these require fairly rapid blood loss to be useful.
- Endoscopy: In this test, a flexible lighted telescope is placed in the mouth or the anus to look for sources of bleeding. Although endoscopy does not diagnose a MD, it looks for other sources of bleeding.
- Infection/obstruction/perforation
- In cases of belly pain, a plain X-ray of the belly may be performed first.
- A computed tomography (CT) scan of the belly may show if there is an infection or blockage.
- Bleeding:
Treatment (“What will be done to make my child better?”)
- Medicine: The initial treatment for patients with a bleeding MD is IV fluid resuscitation, and occasionally blood transfusion. If MD causes infection, perforation or obstruction, antibiotics are usually given.
- Surgery
- Surgery for MD consists of removing it. It may also require removing part of the small intestine next to it and drainage of infected fluid if perforation happened. Surgery can be done using an open or laparoscopic techniques.
- Open surgery: The operation is done using a large vertical cut on the abdomen.
- Laparoscopic surgery: Several small cuts (incisions) are made. Through one of the cuts, a video camera is placed. The surgery itself is done using small instruments placed through the other incisions. The usual number of incisions (cuts) for laparoscopic surgery vary from one (single port umbilical) to a few.
- Open and laparoscopic surgery take about the same amount of time to perform. One benefit of laparoscopy is that other abdominal structures can be examined using the video camera during surgery. Laparoscopy also has lower risks of wound infection.
- Preparation for surgery: Your child will be given fluids, antibiotics, pain medicine prior to surgery.
- Postoperative care
- Activity: Typically, the child is encouraged to walk around as soon as possible.
- Diet: Once function of the intestine returns (as evidenced by passing gas and stool), patients are started on liquids after their surgery then advanced to a general diet.
- Medicines: Your child may need any of the following:
- Antibiotics: To help prevent or treat an infection caused by bacteria.
- Anti-nausea medicine: To control vomiting (throwing up).
- Pain medicine: Pain medicine can include acetaminophen (Tylenol®), ibuprofen (Motrin®), or narcotics. These medicines can be given by vein or by mouth.
- Surgery for MD consists of removing it. It may also require removing part of the small intestine next to it and drainage of infected fluid if perforation happened. Surgery can be done using an open or laparoscopic techniques.
- Risks/Benefits: All abdominal surgeries have risks, including infection, bleeding and damage to nearby structures. Non-operative management is usually not an effective therapy for a bleeding Meckel’s Diverticula, as the likelihood of recurrent symptoms is very high.
Home Care (“What do I need to do once my child goes home?”)
- Diet: Your child may eat a normal diet after surgery.
- Activity: Your child should avoid strenuous activity and heavy lifting for the first 1-2 weeks after laparoscopic surgery, 4-6 weeks after open surgery.
- Wound care: Surgical incisions should be kept clean and dry for a few days after surgery. Most of the time, the stitches used in children are absorbable and do not require removal. Your surgeon will give you specific guidance regarding wound care, including when your child can shower or bathe.
- Medicines: Medicines for pain such as acetaminophen (Tylenol®) or ibuprofen (Motrin® or Advil®) or something stronger like a narcotic may be needed to help with pain for a few days after surgery. Stool softeners and laxatives are needed to help regular stooling after surgery, especially if narcotics are still needed for pain.
- What to call the doctor for: Call your doctor for worsening belly pain, fever, vomiting, diarrhea, problems with urination, or if the wounds are red or draining fluid.
- Follow-up care: Your child should follow-up with his or her surgeon 2-3 weeks after surgery to ensure proper post-operative healing.
Long-Term Outcomes (“Are there future conditions to worry about?”)
- Complications:
- Wound infection: Happens around 3% of the time. Infections may need only antibiotics or may require opening up of the wound depending on how bad the infection is.
- Small bowel obstruction: 3-5% risk in child’s lifetime.
Updated: 11/2016
Authors: Steven L. Lee, MD; Joshua Dale Rousch, MD
Editors: Patricia Lange, MD; Marjorie J. Arca, MD
Meconium Ileus
Condition: Meconium Ileus
Overview (“What is it?”)
- Definitions:
- Meconium: The stool (intestinal contents) that collects in the intestines of fetuses (unborn babies). When the babies are born, they evacuate this stool for the first 24-48 hours, which tends to be thicker and darker than normal baby poop. Afterward, the stools tend to be thinner and lighter.
- Meconium ileus: Blockage of intestine due to abnormally thick meconium at the point where small bowel transitions to large bowel.
- Blockage can happen because the thick meconium does not allow intestinal fluid to go through. Alternatively, blockage can cause the intestine to rupture, twist or not be in continuity.
- Sometimes complications resulting from the blockage may be seen on ultrasounds done to monitor the growing baby inside the mother.
- Epidemiology: Meconium ileus is seen mostly in two populations:
- Cystic fibrosis (CF) patients. CF patients tend to have thick secretions in their intestines as a result of their disease.
- Preterm infants. Sometimes associated with medications to slow down labor.
Signs and Symptoms (“What symptoms will my child have?”)
- Inability to keep feedings down, vomiting, swollen belly, no stool. Sometimes, large intestinal loops may have been seen on prenatal ultrasound, abdominal distension, failure to pass stool. If there is a rupture of the intestine, the baby may be sicker with low blood pressure.
- Conditions that mimic this condition: Other conditions can also cause intestinal blockage including narrowing or discontinuity of intestine, abnormal rotation of intestine, Hirschsprung disease (a disease where the nerves that control intestinal movement do not form completely), incarcerated hernia (intestine caught in a connection between the abdomen and the groin).
Diagnosis (“What tests are done to find out what my child has?”)
- Blood tests: Blood tests to check for CF may be obtained.
- Other tests: Sweat may be tested for concentration of chloride. This will help determine whether someone has CF.
- X-rays: Plain X-rays may give clues as to the cause of intestinal blockage.
- Contrast enema: Water-soluble contrast is instilled through the anal opening and X-rays are obtained to see the anatomy of the large intestine and where the blockage may be. Sometimes, the contrast mixes with the thick stool and allows the stool to be evacuated.
Treatment (“What will be done to make my child better?”)
- Non-operative management
- Non-operative management of meconium ileus can be tried if there are no complications from the blockage (such as intestinal twist, rupture, or discontinuity). Attempts to dissolve the thick meconium can be tried. Water soluble contrast can be instilled into the anus. The contrast can mix and soften the thick meconium, allowing it to be pooped out.
- The infant will have X-rays performed every 8-12 hours to observe progress. If the meconium does not pass completely the first time, but the infant remains stable, the enema can be repeated safely, and after exam by a physician.
- Surgery
- Surgery is needed if an infant fails to respond to enemas and the bowel remains blocked. Surgery is also required if there are complications resulting from meconium ileus such as intestinal rupture, twist or discontinuity.
- The goal of surgery is to relieve the intestine of blockage. If an infection exists, the goal is also to control the infection (for instance, repair a hole in the intestine). What is done in the operating room depends on many factors including the status of the baby (stable vs unstable), size of the baby, and damage to the intestine. Options may include simple flushing of the intestine, removal of an intestinal segment with re-establishment of continuity, creation of a stoma. The surgeon will make a decision of what is the best and safest alternative for the baby while in the operating room.
- Preoperative preparation involves giving fluids and antibiotics.
- Postoperative care: Infants are managed in the neonatal intensive care unit. The infant will likely need the support of a breathing machine (ventilator). It will take days or sometimes weeks for the intestine to gain full function so nutrition will have to be provided through the veins.
- Risks: Risks of operation including anesthesia, bleeding, postoperative infection, damage to internal structures which may require further operation, and recurrence of meconium ileus.
- Benefits: The bowel obstruction from meconium ileus and accompanying complications make the infant very ill. Often surgery is needed to relieve the blockage and help control any existing infection.
Home Care (“What do I need to do once my child goes home?”)
- Diet: The infant’s formula will be determined by many factors such as whether or not s/he has CF and the length of intestine that remains if intestine required resection.
- Activity: Activity should be normal.
- Wound care: By the time the baby is released, s/he should be able to have regular baths. If a stoma remains, you will be trained in stoma care prior to discharge.
- When to call a doctor: Not able to keep down feeds, vomiting (in particular, green or bright yellow vomiting), swelling of the belly, no bowel movements, belly pain, redness or drainage from wound.
- If the infant is diagnosed with cystic fibrosis, they will likely be referred to a specialized group of doctors (lung and gut specialists) to address all aspects of CF care including dietary supplements, exposure restrictions, lung care.
Long-Term Outcomes (“Are there future conditions to worry about?”)
The outcome for meconium ileus treatment has improved to almost 100% survival. If the child required an operation but does not have CF, there is a lifetime risk of intestinal blockage from scarring of about 10-15%. Children with cystic fibrosis are at a much higher likelihood of having pulmonary and gastrointestinal complications as they get older. These will not be discussed here.
Updated: 11/2016
Author: Joanne E. Baerg, MD
Editors: Patricia Lange, MD; Marjorie J. Arca, MD
Meconium Plug
Condition: Meconium Plug
Overview (“What is it?”)
- Definition: Meconium plug is a condition in some newborn infants where the large intestine (colon) is blocked by solid pellets of meconium. “Meconium” is the term used for the stool that collects in the intestines of fetuses (unborn babies). In some babies the stool becomes solidified into hard pellets, causing blockage of the colon.
- Epidemiology:
- The underlying cause meconium plugs is largely unknown.
- A subset of infants with meconium plugs may have Hirschsprung disease (condition where nerves controlling the motility of the intestines) and cystic fibrosis (disease where thick mucus in the lungs and intestines can cause life-long problems), so these diseases should be ruled out.
- It occurs equally in males and females.
Signs and Symptoms (“What symptoms will my child have?”)
- Signs: The newborn does not pass meconium in the first 24 hours of life. There may be swelling of the belly, feeding intolerance and vomiting.
Diagnosis (“What tests are done to find out what my child has?”)
- Labs and tests: When a newborn does not pass meconium, a work-up is started.
- Bloodwork is sent to look for infections, abnormalities in levels of minerals (electrolytes)
- X-rays: Plain X-rays may give clues as to the cause of intestinal blockage.
- Contrast enema: Water-soluble contrast is instilled through the anal opening and x-rays are obtained to see the anatomy of the large intestine and where the blockage may be. If meconium plugs are present in the colon, contrast mixes with the pellets and allows the stool to be evacuated.
- Conditions that mimic this condition: Hirschsprung disease, cystic fibrosis, intestinal atresia, small left colon syndrome (seen in infants of mothers with diabetes), infants whose mothers may have required medicine (magnesium) to stop premature labor, and other causes of newborn bowel obstruction.
Treatment (“What will be done to make my child better?”)
- Contrast enema: Contrast enema helps in both the diagnosis and treatment of meconium plugs. Sometimes, if there are lots of plugs present, repeating the contrast enema may be necessary to clear the intestine of all the plugs.
- The symptoms are relieved and the infant begins to eat and stool normally.
- During the time the newborn is not eating or stooling normally, s/he will be cared for in the neonatal unit. S/he will receive intravenous fluids and may occasionally need nutrition given by vein (total parenteral nutrition or TPN). If s/he is vomiting or the belly is really swollen, a nasogastric tube may be placed into the stomach to drain air and fluid.
- Surgery: Surgery is not needed for meconium plug syndrome.
- In these babies, it is important rule out Hirschsprung disease. Infants with Hirschsprung disease do not have normal nerves in the rectum so the intestine does not allow stool to pass normally. Hirschsprung disease is ruled out by a suction rectal biopsy.
- Suction rectal biopsy: A suction rectal biopsy is the definitive test for Hirschsprung disease. This is usually done at the bedside of the baby and does not require anesthesia. In this procedure, a small instrument (size is slightly larger than a rectal thermometer) is inserted about 2 centimeters into the anal opening. Gentle suction is applied, pulling the rectal lining into the instrument. A small piece of the rectal lining is cut. Three such samples are obtained and sent for microscopic analysis. The pathologist examines the specimens for presence of normal nerves.
- Risks of suction rectal biopsy include bleeding, getting a hole in the intestine and not obtaining adequate specimens.
- In these babies, it is important rule out Hirschsprung disease. Infants with Hirschsprung disease do not have normal nerves in the rectum so the intestine does not allow stool to pass normally. Hirschsprung disease is ruled out by a suction rectal biopsy.
Home Care (“What do I need to do once my child goes home?”)
- Diet: Normal diet for age.
- Activity: No limitations.
- What to call the doctor for: Call for persistent vomiting, swelling of the belly or failure to pass stool.
- Follow-up care: Follow up with the pediatrician at regular scheduled appointments after discharge to be sure the infant is eating normally, stooling and gaining weight.
Long-Term Outcomes (“Are there future conditions to worry about?”)
- The long term outcome for meconium plug syndrome is excellent. Infants have normal eating, stooling and growth. No further evaluation or treatment is needed.
- If the patient is found to have Hirschsprung disease or cystic fibrosis, overall outcomes are different.
Updated: 11/2016
Author: Joanne E. Baerg, MD
Editors: Patricia Lange, MD; Marjorie J. Arca, MD
Mesenteric and Omental Cysts
Condition: Mesenteric and Omental Cysts
Overview (“What is it?”)
- Definitions: Rare condition of the mesentery and omentum due abnormal blockage of lymphatic drainage leading to the formation of fluid filled structures called cysts
- Mesentery: Double layer of tissue connecting the small intestines to the rest of the body. This is where the blood vessels to the intestines are located. Mesocolon is the mesentery to the colon (Figure 1)
 Figure 1. http://images.slideplayer.com/1/273759/slides/slide_11.jpg
Figure 1. http://images.slideplayer.com/1/273759/slides/slide_11.jpg
- Omentum: Folding of fatty tissue extending from the stomach and draping over the large and small intestines (Figure 2)
 Figure 2. https://upload.wikimedia.org/wikipedia/commons/4/44/Sobo_1909_564.png
Figure 2. https://upload.wikimedia.org/wikipedia/commons/4/44/Sobo_1909_564.png
- Lymphatic tissue: Part of the circulatory system that collects extra fluid (called lymph) from various tissues and delivers it back to the venous system
- Epidemiology
- Mesenteric and omental cysts are rare but are seen in 1 in every 100,000 adult hospital admissions, while pediatric literature demonstrates an incidence of approximately 1 in every 11,250 to 20,000 admissions.
- Mesenteric cysts are 4.5 times more common than omental cysts.
- Approximately one-third of cases are found in patients younger than 15 years of age. The mean age in pediatric patients is 4.9 years.
Signs and Symptoms (“What symptoms will my child have?”)
- These masses can be incidental findings on CT scans or during abdominal operations for unrelated conditions.
- Patient complaints are nonspecific. Children with symptoms can have abdominal distention due to enlarging cyst or vague abdominal pain with or without a mass. Sometimes symptoms can mimic intestinal blockage or appendicitis.
- Other symptoms are infection, bleeding, twisting of the bowel leading to loss of blood supply to the intestines (volvulus), ascites fluid inside the belly cavity (ascites) and rupture of the cyst.
Diagnosis (“What tests are done to find out what my child has?”)
- Children with belly pain usually get a regular X-ray of the abdomen first. Unless the cyst causes intestinal blockage, the presence of the cyst will not be seen on regular X-ray.
- Mesenteric and omental cysts will appear as a fluid filled cyst on CT scan and ultrasound.
 Photo courtesy of MJArca 11/2016
Photo courtesy of MJArca 11/2016
Treatment (“What will be done to make my child better?”)
- Medical treatment: No medicine is known to make omental or mesenteric cysts smaller.
- Surgery is recommended for cysts that cause problems such as pain, infection, intestinal twisting.
- Omental cysts are removed.
- Mesenteric cysts may require removal of intestine next to the cyst. If mesenteric cysts are large and removal means removing a really long segment of intestine, partial removal or drainage of the cyst may be needed.
- This can be done the traditional way (“open” or larger incision) or laparoscopic.
- Open: The procedure is done through a cut on the belly.
- Laparoscopy: In laparoscopic procedure, several small cuts (incisions) are made. Through one of the cuts, a video camera is placed. The surgery itself is done using small instruments placed through the other incisions. The usual number of incisions (cuts) for laparoscopic surgery vary from one (single port umbilical) to several.
- Risks for surgery are low but include bleeding, infection, ascites (persistent leakage of lymph fluid in the abdomen), leakage from the bowel (if a portion of the normal bowel is removed) and risks of anesthesia. If the cyst is only partially removed, then the cyst may recur in the future.
- Benefits include removal of the cyst that are causing symptoms.
- Preparation for surgery: Your child will be given fluids, antibiotics, pain medicine prior to surgery.
- Postoperative Care
- Activity: Typically, the child is encouraged to walk around as soon as possible.
- Diet: Patients are started on liquids after their surgery then advanced to a general diet.
- Medicines: Your child may need any of the following:
- Antibiotics: To help prevent or treat an infection caused by bacteria.
- Anti-nausea medicine: To control vomiting (throwing up).
- Pain medicine: Pain medicine can include acetaminophen (Tylenol®), ibuprofen (Motrin®) or narcotics. These medicines can be given by vein or by mouth.
Home Care (“What do I need to do once my child goes home?”)
- Length of admission to the hospital depends on the extent of the surgery. If simple cysts are removed, patients may be discharged the same day as their surgery or the following day. If intestine was removed, then hospital stay will be for a few days.
- Diet: Your child may eat a normal diet after surgery.
- Activity: Your child should avoid strenuous activity and heavy lifting for the first 1-2 weeks after laparoscopic surgery, 4-6 weeks after open surgery.
- Wound care: Surgical incisions should be kept clean and dry for a few days after surgery. Most of the time, the stitches used in children are absorbable and do not require removal. Your surgeon will give you specific guidance regarding wound care, including when your child can shower or bathe.
- Medicines: Medicines for pain such as acetaminophen (Tylenol®) or ibuprofen (Motrin® or Advil®) or something stronger like a narcotic may be needed to help with pain for a few days after surgery. Stool softeners and laxatives are needed to help regular stooling after surgery, especially if narcotics are still needed for pain.
- What to call the doctor for: Call your doctor for worsening belly pain, fever, vomiting, diarrhea, problems with urination or if the wounds are red or draining fluid.
- Follow-up care: Your child should follow up with his or her surgeon 2-3 weeks after surgery to ensure proper post-operative healing.
Long-Term Outcomes (“Are there future conditions to worry about?”)
- Prognosis is excellent after surgery. Most children with mesenteric and omental cysts who undergo surgery have no long-term complications.
- Complications
- Wound infection—occurs rarely
- Recurrence—occurs rarely
Updated: 11/2016
Author: Romeo C. Ignacio, Jr., MD
Editors: Patricia Lange, MD; Marjorie J. Arca, MD
Neck Masses
Condition: Neck Masses: lymphatic malformations and lymphadenitis
Overview (“What is it?”)
- Lymphatic malformations (previously referred to as cystic hygromas) are collections of fluid within abnormal lymphatic channels. They can occur anywhere in the neck, but more often are located on the side. Lymphatic malformations are often detected on prenatal ultrasound and are present at birth. They may be quite large and extend to surrounding areas.
- Lymphadenitis refers to enlargement of lymph nodes. Lymph nodes are organs located throughout the body that help fight infection. Lymph nodes normally get bigger as a response to infection. Infection can be caused by bacteria and other microbes (atypical mycobacteria, cat scratch disease).
Signs and Symptoms (“What symptoms will my child have?”)
- Early signs
- Lymphatic malformations are often detected on prenatal ultrasound and are present at birth. These are soft lumps under the skin that may have the feel of fluid.
- Lymph nodes that are enlarging as a response to infection may be tender or mildly painful. Usually they are flat, firm and moveable bumps under the skin that have a smooth surface.
- Later signs/symptoms
- Lymphatic malformations often grow in proportion with the child, but can increase or decrease in size. Lymphatic malformations can also get infected or bleed into itself.
- Lymph nodes may continue to get bigger as the infection gets worse. The nodes themselves may get infected—get red and form pus.
Diagnosis (“What tests are done to find out what my child has?”)
- Labs and tests: Most of these lesions are diagnosed on history and physical examination.
- Bloodwork: No specific blood tests are needed for lymphatic malformation and lymphadenitis unless an infection is suspected. If the infection is bad enough, an infection cell count and cultures of the blood (to rule out spread of infection into the blood stream) may be obtained.
- Depending on the level of suspicion for a lymph node being large enough to be considered cancer, more blood tests may be obtained.
- Ultrasound is typically obtained and also diagnostic. For lymphatic malformations, an MRI is required to determine the extent of the lesion.
- Bloodwork: No specific blood tests are needed for lymphatic malformation and lymphadenitis unless an infection is suspected. If the infection is bad enough, an infection cell count and cultures of the blood (to rule out spread of infection into the blood stream) may be obtained.
- Conditions that mimic lymphatic malformations include malformations of the blood vessels and inflammation of other congenital malformations of the neck (branchial cleft remnants). Other conditions that can cause lymph node enlargement include cancer. Torticollis (spasm of the neck muscle) can be mistaken for a neck mass.
Treatment (“What will be done to make my child better?”)
- Medicine
- Lymphatic malformations in children may be treated medically. Medicines that have been shown to help shrink certain types of malformations include propranolol or sildenafil. Lymphatic malformations that become infected require antibiotics. This can be given by mouth or through the vein if the infection is bad enough.
- For both lymphatic malformations and lymph nodes that become infected, antibiotics are needed. This can be given by mouth or through the vein if the infection is bad enough.
- Non-operative treatment
- Some lymphatic malformations can be treated with aspiration and injection of medicines that cause internal scarring (sclerosing agents).
- Lymph nodes that got bigger as a response to an infection usually need no treatment. These will slowly get smaller as the infection resolves. They may not get as small as they were prior to the infection. Usually lymph nodes less than 2cm do not need surgery.
- Surgery
- Lymphatic malformations require removal if causing recurrent infection, cosmetic disfigurement, compression of important structures and failed medical and non-surgical therapies.
- Lymph nodes that continue to enlarge or if the cause for enlargement is not certain require removal of the entire node or a piece of the node to figure out what is making the lymph node large.
- If there is an abscess (collection of pus) associated with lymphatic malformation and lymphadenitis, a drainage procedure is needed, where a cut is made over the pus pocket, the pus is drained and the wound is allowed to heal from the bottom up. Sometimes, if the pus pocket is deep, placing a drainage tube or catheter into the cavity is a good option.
- Preoperative preparation: For scheduled operations, a bath or shower the night before or the morning prior to surgery is recommended. For lymphatic malformations, careful evaluation of the extent of the malformation with MRI is required prior to surgical intervention. If cancer is being considered as a diagnosis for lymph node enlargement, a chest X-ray should be obtained to make sure that there are not enlarged nodes close to the heart and airways.
- Postoperative care
- Lymphatic malformations: The length of hospital stay is dependent on how big the malformation is and where it is located. Sometimes, drains are placed after removal of lymphatic malformations. It is often removed one or two days after surgery. Compression garments are often used after surgery for lymphatic malformations. A drain is often left in place and patients may need to go home with the drain still in place. Careful instructions on drain care will be provided prior to discharge.
- Lymph node biopsies are usually done as an outpatient procedure.
- Pain medications will be given. Types of medication include acetaminophen (Tylenol®), ibuprofen (Motrin®, Advil®) or narcotics. These may be taken by mouth or by vein.
- Risks/Benefits: The risks of surgery include bleeding, possible transfusion, infection of the wound, anesthetic risks, damage to surrounding structures (nerves), and recurrence of the lesions. For large lymphatic malformations, there is also risk of injury to large blood vessels and nerves to the upper extremity. Lymphatic malformations have a high risk of recurrence after surgical excision. The benefit of surgical excision is to prevent growth of the lesion and risk of future infection.
Home Care (“What do I need to do once my child goes home?”)
- Diet: Usually regular age appropriate diet.
- Activity: No heavy activity for 2-4 weeks.
- Wound care: Usually no special wound care is needed. Some patients may require drain care.
- Medicines: None except for pain medication.
- What to call the doctor for: Fever worsening pain, wound problems (redness, drainage), shortness of breath, or persistent emesis.
- Follow-up care: With your surgeon in 1-2 weeks after discharge.
Long-Term Outcomes (“Are there future conditions to worry about?”)
For lymphatic malformations, there is a higher risk of recurrence with potential need for additional procedures or surgery. Long-term outcomes after lymph node biopsies are excellent; if cancer is found, a referral will be made to a cancer specialist.
Updated: 11/2016
Author: Steven L. Lee, MD
Editors: Patricia Lange, MD; Marjorie J. Arca, MD
Necrotizing Enterocolitis
Condition: Necrotizing Enterocolitis (NEC)
Overview (“What is it?”)
- Necrotizing enterocolitis (NEC) is an acquired infection or inflammatory disease of the intestines in newborns.
- NEC mostly occurs in premature infants. The more premature and smaller the infant, the higher the risk of NEC. Only about 10% of NEC cases occur in full-term infants.
- Key factors associated with NEC are decreased blood flow to the intestines (ischemia) and infection.
Signs and Symptoms (“What symptoms will my child have?”)
- Early signs of NEC are apnea and bradycardia, temperature instability, not tolerating feedings and lethargy. Other signs include bloody stools and swelling of the belly.
- Later signs/symptoms include abdominal wall discoloration (red or blue), firm abdomen and shock (low blood pressure, heart rate high or low for age).
 Figure 1. Photo courtesy of MJArca11/2106
Figure 1. Photo courtesy of MJArca11/2106
Diagnosis (“What tests are done to find out what my child has?”)
- Labs and tests: The most common blood tests obtained are complete blood count (CBC), electrolytes and blood gas analysis. These may give indications of how severe the infection is. Lab values are followed serially to look for improvement or deterioration.
- Abdominal X-rays will be obtained every few hours to monitor changes such as evidence of intestinal perforation (hole in the intestine).
- Abdominal ultrasound has been used in some centers to look for evidence of non-moving intestine (likely evidence of intestine that may not recover) and fluid in abdomen (evidence of infection or intestinal rupture).
- Conditions that mimic this condition include other causes of infection (blood, urine, lung, etc.). Infections in premature babies will lead to many of the early signs described above.
Treatment (“What will be done to make my child better?”)
- Medicine: The initial treatment for patients suspected of having NEC is to hold feedings and start intravenous (IV) antibiotics. If the diagnosis of NEC is confirmed, then infants are typically treated for 7-14 days.
- Surgery: Surgery is needed for babies with evidence of intestinal rupture (hole in intestine) and/or worsening symptoms of infection. Intervention may be in the form of placing a drain or abdominal exploration. The type of intervention will be individualized and discussed by the treating team.
- Placement of abdominal drain: This is usually reserved for very small and fragile babies with evidence of intestinal rupture (hole in the intestine). The procedure is done at the bedside. A small cut is made in the right lower part of the belly, entering the abdominal cavity to release air and stool. A drain is placed inside the belly, keeping the cut open for several days to allow continued drainage of stool and infected fluid. The drain is inched out about a week after its placement, provided the baby is doing well.
- Abdominal exploration (exploratory laparotomy): Certain conditions warrant a laparotomy including concern that there are dead segments of intestine in the belly. The goal of surgery is to identify these segments and remove them. Most often, a stoma is created, where a segment of intestine is brought out through the belly wall. The stoma is where the baby will stool for a few weeks after surgery. In very select cases, a segment of intestine is removed and the remaining intestine is put back together.
- Preoperative preparation: Patients will continue on antibiotics and may need transfusions of blood products prior to surgery.
- Postoperative care: These patients are usually very sick, requiring a breathing tube and a ventilator for support. Medicines to support blood pressure may be needed. Transfusions of blood products may be needed. Patients will remain on antibiotics after surgery. Patients will not be fed for a period of time after surgery. Patients may require additional procedures.
- Risks/Benefits: Patients who improve with antibiotics do not need surgery. However, when patients are clinically getting worse or have signs of intestinal rupture on X-ray, surgical intervention is required. Sometimes, the entire intestine may be damaged by the infection leading to a poor prognosis and maybe death.
Home Care (“What do I need to do once my child goes home?”)
- Diet: Will be based on how much intestine is remaining.
- Activity: Normal newborn/premature activity.
- Wound care: By the time baby is home, no special wound care is needed and the baby is bathed normally. If the baby has a stoma, stoma care and management will be taught to parents prior to discharge.
- Medicines: Mostly for issues related to prematurity.
- What to call the doctor for: Persistent vomiting (especially if green or bright yellow), no stools, watery stools, swelling of the belly, fever.
- Follow-up care: Surgery follow-up in 1-2 weeks. Routine NICU follow-up per institutional schedule.
Long-Term Outcomes (“Are there future conditions to worry about?”)
Long-term outcomes are based the amount of intestines remaining after surgery. Another potential condition is the development of scar tissue within the abdomen (adhesions) that can lead to intestinal blockage.
Updated: 11/2016
Author: Steven L. Lee, MD
Editors: Patricia Lange, MD; Marjorie J. Arca, MD
Neuroblastoma
Condition: Neuroblastoma
Overview (“What is it?”)
- Neuroblastoma is a type of tumor that arises from cells of the sympathetic nervous system and adrenal gland.
- The nervous system consists of the brain, spinal cord and nerves. The sympathetic system is a part of the nervous system that helps control adjustments in heart, muscle or intestinal activity, especially during stressful events.
- The adrenal glands are organs located on top each kidney. The adrenal gland have cells similar to the sympathetic system that make chemicals called epinephrine (adrenaline) and norepinephrine (noradrenaline). These chemicals are important in the response to stress situations.
- Epidemiology
- Neuroblastoma is seen mostly in children. It is the third most common childhood cancer, after leukemia and brain tumors.
- More than 600 new cases are diagnosed in the United States each year.
- The average age at diagnosis is 2.5 years with 40% being diagnosed before age one.
- Neuroblastomas are associated with some congenital abnormalities and genetic diseases such as Hirschsprung disease, central hypoventilation and neurofibromatosis.
- Since neuroblastomas arise from cells of the nervous system, it can occur in any area with sympathetic nerve tissues, including the adrenal gland (46%), the chest next to the spine (15%), the pelvis (4%), and the head and neck (3%).
Signs and Symptoms (“What symptoms will my child have?”)
- The symptoms of neuroblastoma vary according to the location of the main tumor and whether or not it has spread to other places in the body.
- When the tumor arises inside the belly, there may be a mass or firmness felt during a physical exam.
- When they occur in the chest, it may compress the windpipe (or trachea, which is a major airway in the neck and upper chest) and create coughing or difficulty breathing.
- If it is near the spinal cord, it can create a loss of sensation or motor function below the level of involvement.
- Spread to the lymph nodes can create enlarged lumps or bumps on the body, while spread to the bone marrow can create fatigue and an inability to fight infection.
- Some common symptoms that children can experience with neuroblastomas regardless of its location include weight loss, fever, abdominal disturbances, diarrhea, high blood pressure, irritability, pain of bone and joints, or inability to stand up or not walk.
Diagnosis (“What tests are done to find out what my child has?”)
- Bloodwork
- Neuroblastomas can secrete different hormones. Blood and urine samples may be tested for the presence of such hormones.
- When these levels are elevated, they can be used to follow the response of the disease to treatment or to watch for recurrence.
- Imaging studies
- Some cases of neuroblastoma can be identified during prenatal ultrasound.
- Usually when there is belly swelling, plain abdominal X-rays are obtained first. X-rays are energy beams that go through the body onto a film, making a picture on the film.
-
- Ultrasound may be used to assess for a neck or abdominal mass. Ultrasound uses sound waves to create images and pictures.
- CT scans or MRIs may also be used to identify the mass or to check for metastasis.
- Computed tomography (CT) scans: Detailed pictures of the chest or abdomen are taken, reconstructed in different views to get a better picture of the liver mass.
- MRI (Magnetic Resonance Imaging): Uses a magnet, radio waves and computer to obtain images of organs in the body. MRI does not use radiation.
- Bone scans and bone x-rays can show the presence of bone metastases.
- Iodine-123-labeled metaiodobenzylguanidine (MIBG), a radiolabeled marker that is processed by the adrenal gland, is a nuclear medicine test that is useful in identifying the tumor and metastases.
- If metastasis of the bone is suspected, needle aspiration of the bone marrow may be recommended.
- Biopsy: A biopsy or taking a piece of tissue from the mass, may be needed to make a definite diagnosis by looking at the tissue under a microscope.
Treatment (“What will be done to make my child better?”)
- Staging: In all types of cancer, it is important to determine if the cancer is isolated or has it spread through the body. The treatment is dependent on the stage of the cancer.
- In neuroblastoma, staging is done to look at whether the tumor can be completely removed without causing significant harm to the surrounding organs and the child. Staging will also be done to see whether there is cancer spread in organs other than where the primary cancer is seen.
- A pediatric oncologist (doctor that specializes in treating pediatric cancer) will guide you through the types of medicines and radiation to be used.
- Medicine: Chemotherapy are drugs that are especially aimed at destroying neuroblastoma cells, are used either before AND after surgery or just after surgery. These are given through the vein.
- If the tumor is too big, situated in a dangerous place for the child’s safety, or there is tumor spread, chemotherapy may be used to decrease the size and tumor burden before surgery to remove the tumor.
- If the tumor is too close to certain organs (close margins) or if the tumor has aggressive characteristics, chemotherapy may be needed after surgery.
- As chemotherapy attacks cells in the body that are rapidly dividing, it may also affect normal cells in the body that rapidly divide.
- Common side effects of chemotherapy include hair loss, mouth sores, loss of appetite, nausea, vomiting, diarrhea, constipation, increased chance of infections, easy bruising or bleeding and fatigue. Most of these effects are short-lived and will go away after treatment.
- Radiation therapy may also be used if any tumor cells are left behind after surgical removal of the mass.
- Radiation therapy uses high-energy rays to kill cancer cells. Although it is administered locally to the tumor, normal cells that surround the tumor may be affected as well.
- Possible short-term effects of radiation include nausea, diarrhea, fatigue, sunburn changes to the skin and hair loss.
- Surgery: Due to the rare and complex nature of these tumors, treatment should be performed at centers/hospitals where surgeons are very familiar with neuroblastoma. Tumors are removed if they are able to completely resected safely.
- The mass/tumor can usually be resected at the time of diagnosis in about some patients but some have tumors that are too large to be removed right away and will get chemotherapy first.
- Preoperative preparation: Your child will require general anesthesia for any surgical procedure so will have to stop eating several hours before the surgery. A shower or a bath the night prior or the day of surgery helps cleanse the skin to decrease wound infections. Certain labs may be drawn to check blood count levels and to check the function of the liver.
- Postoperative care: Your child will likely remain in the hospital for several days following the surgery in order to provide good pain control and intravenous fluids. Once s/he is eating well and able to take medications by mouth, they will be discharged.
- Central line placement (Port-A-Cath® or Broviac® Catheter) will likely be necessary to give chemotherapy drugs before or after removing the liver tumor.
- Metastases (pieces of tumor that have spread to other parts of the body, usually the lung) will need to be controlled.
- Risks/Benefits
- The main risks of surgery are bleeding and infection. Your child will likely have their blood type checked before surgery in case a blood transfusion will be necessary. They will also be given antibiotics before and maybe after surgery to help reduce the chance of infection.
- The other risk of surgery is not getting all the tumor out. This may mean that your child will need additional surgeries in the future or additional chemotherapy to rid the liver of cancer cells.
- There are risks to the drugs used to treat the tumor as well and include heart and kidney problems, lowering of blood cells, developing other tumors and the risk of infection (usually from the central line).
Home Care (“What do I need to do once my child goes home?”)
- Diet: Your child will likely be able to resume a normal diet without restrictions.
- Activity: Depending on the extent of surgery, your child might need to take it easy for a few weeks after surgery. Children tend to recover faster than adults so they may be able to return to school and light-duty activities within a week or two.
- Wound care: Your surgeon should inform you of any specific wound care and whether or not you can get the incision wet. Call your surgeon if there is any redness or drainage from the incision or if your child has any fevers. You will also be given instructions in how to care for the central line.
- Medicines: You may be given a prescription for pain medications. Depending on the tumor, your child may need to return to the hospital or clinic to receive chemotherapy (drugs that attack cancer cells).
- What to call the doctor for: Call your surgeon for fevers (greater than 101° Fahrenheit), redness or drainage from the incision or for any vomiting or diarrhea.
- Follow-up care: You will generally need to see your surgeon one to two weeks after your surgery and will also have a follow up with your oncology doctor.
Long-Term Outcomes (“Are there future conditions to worry about?”)
- Prognosis
- Neuroblastomas that are 1) diagnosed under the age of 18 months, 2) located in the chest, neck or lower spine and 3) do not have lymph node involvement all have more favorable outcomes. In these low-risk groups, there is a 90% long-term survival rate.
- In cases where the tumor is 1) too large, 2) there is lymph node involvement or 3) distant metastasis (spread of cancer to other organs), outcomes may not be as good and chemotherapy and/or radiotherapy may be the only option for treatment.
- Your child will require long-term follow up with the oncologist as well as the surgeon to monitor for tumor coming back and for possible side effects of the treatment.
- Although long-term outcomes depend on the stage of neuroblastoma and the response to treatment, many children have a good chance of long-term survival.
- Follow-up care after treatment for neuroblastomas is important to assess for recurrence of the tumor. Doctors will likely order follow up blood work, CT scans, PET scans, MRI or ultrasounds on a regular basis. It is important that new symptoms be reported to doctors right away.
- Long-term effects of chemotherapy depend on which drugs are used for therapy. Potential long-term side effects include hearing loss, heart damage, numbness and/or tingling, weakness or pain. Some drugs may also increase the risk of later developing a blood cancer termed ‘leukemia’.
- Long-term effects of radiation therapy include curvature of the spine, neurologic problems such as paralysis, numbness, and an inability to spontaneously void if the tumor is located on the spine. Hypothyroidism may result from radiation to the head and neck. Damage to the ovaries may occur in girls with radiation to the abdomen.
References
- Cheung, Nai-Kong; Cohn, Susan; Neuroblastoma. Pediatric Oncology 2005.
- Imbach, Paul; Kuhne, Thomas; Arceci, Robert; Pediatric Oncology: A Comprehensive Guide 2006.
- Moore, S.W.; Satge, D; Sasco, A.J.; Zimmermann, A.; Plaschkes, J.; The epidemiology of neonatal tumors: A report of an international working group. Pediatric Surgery International 2003.
- http://www.cancer.org/cancer/neuroblastoma.
Updated: 11/2016
Authors: Romeo C. Ignacio, Jr., MD; M. Ganyo, MD
Editors: Patricia Lange, MD; Marjorie J. Arca, MD
Omphalocele
Condition: Omphalocele, exomphalos
Overview (“What is it?”)
- Definition
- An omphalocele is an opening in the middle of the belly where the muscle and skin is not present. Instead, the organs are covered by a thin transparent sac. The umbilical cord (belly button) is located in the center of the sac.
- Giant omphalocele: If the opening is greater than five centimeters in diameter and contains mostly liver, it is a giant omphalocele. Infants with giant omphaloceles have more problems with breathing, feeding and overall survival compared to those with smaller defects.
 Figure 1. Courtesy of M. Arca 11/2016
Figure 1. Courtesy of M. Arca 11/2016
- Epidemiology:
- Incidence: Between 1 in 3,000 – 10,000 live births
- Omphaloceles are associated with older mothers.
- In some cases, omphalocele can be associated with chromosomal syndromes (abnormal genes).
- 20-50% of babies with omphaloceles are born with cardiac abnormalities.
Signs and Symptoms (“What symptoms will my child have?”)
- Early signs: Most omphaloceles are diagnosed during prenatal ultrasound. If the omphaloceles are small, they may be diagnosed after the baby is born.
Diagnosis (“What tests are done to find out what my child has?”)
- Prenatal Studies: Once the baby inside the mom is suspected or found to have omphalocele, other studies may be needed. Not all of these may be needed:
- Blood test: Alpha fetoprotein is a substance that is elevated in the blood stream.
- Ultrasound: The mother will have frequent ultrasounds to evaluate the growth of the fetus and make sure that the sac covering the hole remains intact
- Magnetic Resonance Imaging (MRI): Some centers obtain an MRI to evaluate the baby’s heart, lungs and other organs.
- Amniocentesis: Fluid from inside the uterus may be aspirated to look for chromosomal abnormalities.
- Conditions that mimic this condition: Other defects of the belly wall such as gastroschisis, extrophy may mimic omphalocele.
Treatment (“What will be done to make my child better?”)
- A baby with omphalocele should deliver in a hospital that has ready access to surgeons and specialists that can take care of the baby right away (usually a dedicated children’s hospital). Your obstetric doctor will discuss options about delivery. In a baby with large omphalocele, a Caesarian section (C-section) is recommended, as passage through the birth canal can injure the liver, causing bleeding. Ideally, the parents can meet with surgeons and infant specialists before the baby is born to get an idea where and how your child will be cared for.
- After initial stabilization, a thorough exam is done and investigations are arranged to evaluate for other associated abnormalities. These include an echocardiogram to look at the structure of the heart, a chest X-ray and further chromosome analysis.
- Surgery
- The size of the defect, the amount of liver and intestines that are out into the sac, the size of the baby and presence of other abnormalities determine the surgical approach.
- Primary closure: In general, if the defect is small and the baby is healthy, the muscle and skin can be closed within a couple days after birth.
- Delayed closure: When the hole is large, the size of the belly cavity is correspondingly small. Replacing all the organs that have been out of the belly all at once creates a tight space that may slow down the blood flow to these organs.
- In these cases, the sac covering the defect is encouraged to mature into regular skin. This process takes months. During skin formation, there is a chance that infection can occur. The sac is protected by medicines that fight infections. During the first few months or weeks the sac is fragile and can tear. This creates a situation where surgery is needed to place temporary coverage on the exposed organs.
- When the infant has grown to the degree that the organs fit into the abdominal cavity, the muscles can be closed. Closure usually takes several surgeries spaced between months. During this time, infants with large omphaloceles may establish full feeds. They can eat and grow.
- Preoperative preparation
- For a small omphalocele, closure is done a few days after birth. The infant will receive antibiotics through the vein to decrease infection.
- For a large omphalocele, closure is done months after birth and on a scheduled basis. At this time, there is usually mature skin covering the omphalocele sac. A bath or shower the night prior to or the morning of the operation is encouraged. The infant will receive antibiotics through the vein to decrease infection.
- Postoperative care: After an omphalocele is closed, the infant is cared for in a monitored setting. Feedings will resume once intestinal function returns.
- Pain medicine: Pain medicine can include acetaminophen (Tylenol®), ibuprofen (Motrin®) or narcotics. These medicines can be given by vein or by mouth.
- Benefit: The benefit of surgery is having organs protected by the muscle and skin. The benefit of the delayed closure approach is that often the infant can be discharged from hospital and return for closure as a planned, elective admission.
- Risks: Returning organs to a tight abdominal space can decrease the blood flow to the organs. This should be monitored closely whether the repair is done days or months after birth. Wound infection, need for a post-op ventilator, bleeding, damage to internal organs that may need repair, as well as anesthesia risk are all risks of surgery.
Home Care (“What do I need to do once my child goes home?”)
- Care of infants with omphaloceles is more complicated if they have problems with other organs such as the heart and lungs.
- Diet: If the infant is ready to go home, in general, they will be eating normally. If they have heart or lung problems, they may need to have supplemental feedings by a tube that goes into the stomach or nutrition by vein. Supplementation is more the exception than the rule.
- Activity: In general, normal activities according to the child’s developmental stage should continue. If the child has a giant omphalocele that is still maturing, it is advisable to have a protective device over the omphalocele. This is usually fashioned in the hospital by occupational therapy.
- Wound care: The surgeon will give instructions for wound care. If a complete closure is done, the wound would be ready for baths upon discharge.
- Medicines: By the time of discharge, minimal oral pain medication such as Tylenol® can be administered. Postoperative pain should have almost resolved.
- What to call the doctor for: Wound redness, drainage, fever. Vomiting, especially green vomiting, can indicate intestinal obstruction and requires immediate attention.
- Follow-up care: If the post-operative course is uneventful, the infant can see the surgeon in one or two weeks after discharge in the office.
Long-Term Outcomes (“Are there future conditions to worry about?”)
- Infants with omphaloceles can have a long chronic recovery phase. Comorbidities that exist in addition to the omphalocele influence survival.
- The size of the defect influences outcome and some report a 25% mortality rate for giant omphaloceles. Death is usually due to respiratory failure, infection or prolonged intravenous feedings (TPN) that damage the liver. Prognosis is good for isolated small omphaloceles and no other comorbidities. Survival rates are between 75-95% for these infants.
Updated: 11/2016
Author: Patricia Lange, MD
Editor: Marjorie J. Arca, MD
Ovarian Torsion
Condition: Ovarian Torsion
Overview (“What is it?”)
- The ovary is an organ in females that is important in reproduction. There are usually two ovaries (right and left) located in the lower belly, on either side of the womb (uterus).
- The ovary makes hormones for development of female organs and releases an egg once a month.
 Figure 1. https://www.womenshealth.gov/publications/our-publications/fact-sheet/images/ovarian-cysts-lg.jpg
Figure 1. https://www.womenshealth.gov/publications/our-publications/fact-sheet/images/ovarian-cysts-lg.jpg
- Ovarian torsion is when the ovary twists around its stalk. The blood vessels to the ovary are located in this stalk. Twisting cuts off the blood supply to the ovary, causing the ovary to possibly die. The Fallopian tube (tube that brings egg from the ovary to the womb) can also be involved in the twist.
- Epidemiology: Ovarian torsion is the fifth most common emergency of the female reproductive organs.
- Etiology (cause): Sometimes a mass or cyst in the ovary can cause twisting. If the stalk of the ovary is long, it may also lead to torsion.
Signs and Symptoms (“What symptoms will my child have?”)
- Early symptoms: Pain in the lower belly, usually sharp and sudden when it starts.
- Later symptoms: Worse pain that is constant, vomiting, nausea
- Conditions that mimic this problem: Appendicitis, urine infection, kidney stones, gastroenteritis, pregnancy
Diagnosis (“What tests are done to see what my child has?”)
- The tests ordered for ovarian torsion are tests that are generally done to find out causes of belly pain.
- Blood work: Blood test to look at the infection count may be ordered
- Urine test: Urine test to look for infection, rule out pregnancy
- Abdominal X-ray: A regular X-ray of the belly may be ordered to look for problems in general, such as constipation.
- Ultrasound: An ultrasound uses sound waves to create an image. It does not use radiation. It is useful in looking at the ovary and also the appendix. The bladder has to be full when the ultrasound is being performed, so the child needs to drink a lot or get fluids through the vein and not pee before the ultrasound is done. The ultrasound may give an idea if there is a cyst in the ovary, lack of blood flow to the ovary.
Treatment (“What will be done to make my child better?”)
- Medical management: There is no medicine that can untwist the ovary. However, pain medications such as narcotics may be given if the child has a lot of pain.
- Surgery: Surgery is the only treatment for ovarian torsion. The goal of the operation is to untwist the ovary and Fallopian tube and restore blood flow to these organs.
- This can be done using open or laparoscopic approach.
- In a laparoscopic procedure, small cuts are made on the belly. Through one of the cuts, a video camera is placed. The surgery itself is done using small instruments placed through the other incisions. The usual number of incisions (cuts) for laparoscopic surgery vary depending on the situation
- In an open approach, a cut is made on the bikini line or midline below the belly button.
- The ovary usually looks blue, swollen and may have clots inside even after it is straightened out.
- Often it is difficult to see if there is an associated mass or cyst that caused the torsion.
- Preoperative preparation: This surgery is usually an emergency, and there are no preparations needed.
- Postoperative care: Most patients are discharged the day after surgery. The child should be able to tolerate liquids before leaving.
- Risks: Bleeding, infection, pain. Recurrence of the torsion is rare. The ovary may live or die after it is untwisted, depending on how long it suffered without blood flow. It is recommended that the ovary should remain inside because at the time of the operation, no one can predict if the ovary will live or die.
- Benefits: Blood flow to the ovary is restored and the ovary may be saved.
- This can be done using open or laparoscopic approach.
Home Care (“What do I need to do once my child goes home?”)
- Diet: Most patients are able to eat a general diet.
- Activity: General guidelines: For open procedures, no gym for 2-4 weeks. weight restriction of 10 pounds for six weeks. For laparoscopic surgery, no gym for 1-2 weeks, weight restriction of 10 pounds for one week, then no weight restriction. Ask your surgeon for specific recommendations.
- Wound care: The patient can shower in three days but may want to wait 5-7 days after surgery before soaking the wound.
- Medicines: Medication for pain such as acetaminophen (Tylenol®) or ibuprofen (Motrin® or Advil®) or something stronger like a narcotic may be needed to help with pain for a few days after surgery. Stool softeners and laxatives are needed to help regular stooling after surgery, especially if narcotics are still needed for pain.
- What to call the doctor for: Problems that may indicate infection such as fevers, wound redness and drainage should be addressed.
- Follow-up care: The patient should be seen by a surgeon or pediatrician/family practice doctor at least once to check the surgical wound. The surgeon will likely obtain an ultrasound a few weeks after surgery to see if there is a mass or cyst in the ovary that caused the torsion and if the ovary remained alive or scarred down.
Long-Term Outcomes (“Are there future conditions to worry about?”)
Surgeons try to save the ovary after torsion because the future ability to have children (fertility) decreases if an ovary and/or a fallopian tube is removed. If there is a cyst or a mass that is seen on follow-up ultrasound, this may require another operation. Overall, girls do very well after ovarian torsion.
Updated: 11/2016
Author and Editor: Marjorie J. Arca, MD